
Why Was Moderna Allowed to Use A Toxic mRNA Dose?
The data that proves Moderna used a deadly dose and the psychopathy that led to the choice to use it

Story at a Glance:
•One of the major problems facing mRNA technology was finding a dose that was strong enough to elicit the desired effect but simultaneously not unbearably toxic. Moderna in turn chose a dose that was 3.3X greater than what even Pfizer felt was safe enough to use.
•Since the vaccines hit the market, numerous datasets have shown the Moderna vaccine is roughly 50% more likely to injure recipients (which includes deaths, miscarriages, and birth defects). Despite this, no regulator has done a basic comparison on the safety of the vaccines.
•Steve Kirsch recently got access to a country-wide dataset on deaths following vaccination. It showed clearly and unambiguously that the Moderna vaccine caused 30% more deaths than Pfizer’s. Additionally, it also showed that Pfizer’s vaccine raised the risk of death by 34% and that both vaccines had minimal efficacy in preventing COVID-19 deaths.
•Moderna’s decision to bring a toxic mRNA dose to market reflected the corrosive culture at this startup, which swindled billions from investors over false promises of the miracles of mRNA and fired any employee who did not repeat the mantra, “mRNA gene therapies are safe and effective.” Likewise, Moderna’s approval and protection once on the market go hand in hand with the government's heavy financial investment in Moderna.
One of the most common questions I received at the start of the COVID-19 vaccine rollout was if it was better to take Pfizer, Moderna or to wait for J&J’s to come out. Given all the potential risks of the mRNA technology (e.g., of it not breaking down, it potentially integrating into the genome, or it having a high theoretical risk for causing cancer, autoimmunity, and blood clots—all of which there was still no public data on), my typical advice was to wait for J&J’s likely safer one to come out as that would give them more information on the risks and benefits of each one and simultaneously to provide them with early treatment options for COVID-19 so they didn’t need to be as concerned about catching the infection.
Note: each of the sources I linked to above demonstrates why it was possible to know this risk existed prior to the vaccine rollout.
Based on their comparative designs and the reports I received, I suspected Moderna was the worst. For example, someone I knew who developed a common debilitating autoimmune condition after Moderna was told by their rheumatologist that they had seen the exact same thing happen in multiple patients after Moderna, while someone I know who had a sudden expected tendon rupture was likewise told the same thing by their orthopedic surgeon. Unfortunately, it wasn’t possible to come to a clear conclusion here as the majority of the people who shared their adverse reports with me (and I compiled here) knew it was Pfizer or Moderna but weren’t sure which, and since far more Pfizer vaccines were given in the United States that it became quite hard to know if proportionally I was receiving more reports of severe injuries from Moderna.

Note: I similarly saw the fewest injuries from J&J, but within samples I took of people I knew who took each, J&J seemed to have a comparable if not higher acute injury rate than the mRNA vaccines (whereas the mRNA seemed to be worse in the long term).
However, despite the potential issues with Moderna’s vaccine, I’ve largely focused on Pfizer’s malfeasance throughout the pandemic. This essentially was because:
•Pfizer’s vaccine was FDA approved, so it was possible to get significantly more information on it (e.g., through FOIA requests—whereas it is only been fairly recently that we’ve been able to get records of the severe injuries that occurred throughout Moderna’s clinical trials).
•Pfizer has a long track record of unscrupulous and criminal behavior (e.g., their behavior now is very similar to what these and these Pfizer employees blew the whistle about within Pfizer in the past).
Therapeutic Dosing
Since most pharmaceutical drugs, are to some extent toxic, a key challenge in making every drug is to figure out how much to give in order to achieve the desired effect without giving too much and creating unwanted toxicity.

Note: I wrote much more about how we determine the correct dose (one of the critically important Forgotten Arts of Medicine) here.
With some substances, there is a wide distance between the two (e.g., while people can get ill from drinking way too much water, this only happens in rare cases where someone is intentionally drinking way too much water). Conversely, some drugs have a very narrow therapeutic index, and hence need to be given under controlled circumstances (e.g., chemotherapy being given intravenously) that ensure the dose stays within its therapeutic index. Furthermore, many drugs have a low enough threshold for toxic effects that no “therapeutic window” exists (e.g., chemo), and instead a dose has to be chosen which accepts minor or moderate effects and simply keeps the dose low enough to avoid severe and fatal side effects or one that accepts a minority of patients with never be able to get a safe dose and that they will simply be collateral damage.
Note: in other cases, the toxicity is simply too high and the drug is abandoned or regulated to only be used in very special circumstances.
When I looked into the mRNA technology, I initially thought that despite it holding immense potential for profitability (as thousands if not millions of costly proprietary drugs could be made with the platform), it wouldn’t go anywhere because it had insurmountable dosing issues. Specifically:
•There was no way to reliably ensure the desired dose of the final gene product (whatever protein the mRNA made) could be made, as cells would break down the mRNA at different rates and different people would have different parts of the body uptake the mRNA (which in turn would produce the mRNA at different rates).
•The body rapidly breaks down mRNA, so a fairly high dose of mRNA had to be given to ensure that enough remained to produce the desired protein.
Note: to some extent, this problem was “solved” through pseudouridation (explained in further detail by Dr. Malone here), as pseudouridation blocks the body from breaking the mRNA being broken down. Unfortunately, that created a much larger issue by causing the mRNA (and hence its spike protein production) to persist in the body indefinitely, both significantly injuring many and preventing the immune system from being able to respond to new variants with spike proteins differing from the artificial one in the vaccine.
•Artificial mRNA (and the lipid nanoparticles that delivered it) had significant cellular toxicity to the body. Because of this, decades ago, early pioneers in the field (e.g., Robert Malone) eventually abandoned the technology because he’d concluded it was simply not possible to overcome its cellular toxicity. More recently, a 2016 article showed that this had Moderna had run into this roadblock as well to the point it was too dangerous to even conduct preliminary human trials. In turn, my suspicion was that, at least initially (e.g., the first decade of commercial use), the only viable use for mRNA technology, would be as an experimental technology for otherwise fatal diseases (e.g., certain genetic defects or cancers) where the severe toxicity of the mRNA was counterbalanced by the fact the patient was otherwise expected to die.
•Since it is a gene therapy with numerous steps in its production, this technology (which, due to its very narrow therapeutic index, requires precise manufacturing) would be nearly impossible to manufacture, especially when done at scale. This again was why I thought it would only be possible to use it in a very narrow context (e.g., a rigidly controlled therapy for a subset of cancer patients).
Note: as discussed in a recent article, major production issues in the mRNA vaccine process resulted in very different mRNA lots.
The “solution” eventually identified was to present the technology as an emergency vaccine, thereby allowing it to gain the advantages of “emergency” medical interventions (e.g., a lower bar for approval and complete immunity from injury lawsuits) and those afforded to vaccines where efficacy (or more specifically an antibody response) was prioritized over safety. For historical context:
When designing the HPV vaccine, Merck realized that it was difficult for the body to develop an immune response to the HPV antigen (which I suspect was due to the body being designed to resist developing autoimmunity and the vaccine’s antigen having similarities to human tissue). To solve this problem, Merck used a much stronger adjuvant.
This “worked” and ensured the vaccine reliably produced an immune response in its clinical trial subjects—but also caused the vaccine to have a very high rate of severe side effects in those who received it. However, since the FDA prioritized “efficacy” this trade-off was accepted and ever since then the FDA and CDC have worked hand-in-hand to cover up the immense number of injuries that have been caused by the HPV vaccine.
Note: one of the major questions everyone has had about the COVID vaccine is why a design was chosen that mass produced the most toxic and rapidly mutating part of the virus (its spike protein) within the body—thereby both guaranteeing that the vaccine would injure its recipients and rapidly stop being effective as a vaccine (since the virus would no longer have the same spike protein).
The most benign answer I can give is that “Operation Warp Speed” was a race to capture the bonanza afforded to whoever could bring the first COVID-19 vaccine to the market (or alternatively bring a vaccine to market before natural immunity had eliminated COVID—something seen in African countries that never vaccinated), and that the design Pfizer and Moderna chose (using an existing gene therapy platform to quickly produce the most reactive part of the spike protein and then overproduce it within the body) was the fastest way to get a reactive one to market. Likewise, if you look at the history of the Moderna vaccine, the spike protein was chosen as the vaccine antigen in January 2020 at a time when the inherent toxicity of the spike protein was not yet known and it is my suspicion that by the time this was recognized, Moderna was not willing to abandon the antigen because it was too late in the race for a vaccine for them to chose a new design.
The more nefarious explanation was that the known issues with this vaccine would pave the way for a continuous line of new products (e.g., since the virus would continually evolve resistant to the existing vaccine antigen, that gave a justification for bringing mandatory boosters to the market, and likewise the wide range of injuries these vaccines created a large market for therapeutics to them—something companies like Pfizer, in turn have already invested in).
Dosing of the mRNA Vaccines
Given all the previous, I was immensely curious about how the vaccines would be dosed. In light of past precedent, I assumed a high dose would be chosen that guaranteed efficacy (specifically the desired antibody response—something which does not necessarily correlate with immunity) at the expense of safety.
Similarly, from the start, I was immensely curious about the lipid nanoparticle design for the vaccine (as it also had to surmount a variety of technical and safety challenges), so when leaked regulatory documents detailed what was in Pfizer’s vaccine, I dove into the details and saw that a specific formulation had been chosen as it appeared to be the only one that allowed the vaccine to work (by getting mRNA inside cells). As no mention of safety for the lipid nanoparticle was mentioned in the regulatory documents, I assumed safety had not been a consideration in choosing it, and that the lipid nanoparticle likewise would have a variety of issues (e.g., it contained PEG, something many are allergic to).
When the mRNA COVID vaccines (which were very similar) finally came to market, I then went and checked what dose each had used.
Each dose of Pfizer’s contains 30 micrograms of vaccine. Moderna went with a much larger dose of vaccine, 100 micrograms [and 50 micrograms for its boosters]. It means the company is using a little more than three times as much vaccine per person as Pfizer is. While Moderna’s initial results didn’t seem to justify the much larger dose, data suggest the protection the company’s vaccine generates is declining at a slower rate than Pfizer’s is; some experts believe the higher dose may be at least partially responsible.
Given that Pfizer is notorious for putting unsafe products onto the market that, for the sake of efficacy, are dosed too high, it immediately caught my eye that another (relatively unknown) company that had no existing products was using a much higher dose than what Pfizer was willing to gamble on. To me, this suggested that Moderna was willing to take a much larger risk to get an approved vaccine to market (as there was no existing business to lose if they got sued and they desperately needed a viable product), and that Moderna may have been a pump and dump operation.
This to some extent was confirmed by Pfizer’s initial phase 1/2 trial, where the 100 mcg dose (Moderna used) was terminated midway due to its side effects:
Based on the tolerability profile [ie. reactogenicity reported] of the first dose at the 100 µg dose level and the second dose of 30 µg, participants randomized to the 100 µg group did not receive a second vaccination.
Note: there is some evidence that suggests mRNA lots with different doses (and thus toxicity) were released onto the market in a manner which made it possible to track which doses created lots that were too hot (and hence needed to be avoided in future products).
Moderna’s Increased Toxicity
In turn, as time passed, more evidence accumulated suggesting that Moderna's higher dose was indeed more dangerous.
First, when the Fraiman paper analyzed the clinical trials for Moderna and Pfizer (which got the vaccines approved), its authors found Moderna had a 50% higher rate of serious adverse events of special interest (AESI) than Pfizer vs. their respective placebos (15.1x vs 10.1x).
Likewise, when I looked at the more common side effects (e.g., headaches, joint pain, and fatigue) in the Pfizer trial and the Moderna trial, I found that they were roughly 30% more common in Moderna’s trial.
Second, when death rates were analyzed from the vaccine adverse event reporting databases, they found Moderna caused 1.3 to 1.5 as many injuries. For example, when the Moderna vaccine was compared to the Pfizer vaccine:
•Dennis Rancourt’s VAERS analysis found a 1.3X increase in death.
•Steve Kirsch’s VAERS Analysis found a 1.3X increase in death.
•Norman Fenton showed that the UK Yellow card system had a 1.5X increase in adverse events that were reported.
•The V-Safe Data showed a 1.8X increase in adverse events.
Third, Igor Chudov discovered some concerning pregnancy data. Specifically:
•At the CDC’s October 2022 ACIP meeting, (ACIP is the outside committee of “experts” who are responsible for “independently” giving evidence-based recommendations for which vaccines should be administered throughout America), ACIP shared some of the V-safe data to assure the public the vaccine was safe for pregnant mothers. However, as Igor noticed, it also showed that for mothers who took the vaccine, 3.3% of the 12,751 women who took Pfizer miscarried before 20 weeks, whereas 4.8% of the 8,365 women who took Moderna miscarried—a result Igor then demonstrated was scientifically significant.
Given the size of this sample, this demonstrates that the higher Moderna dose increased one’s risk of a miscarriage by 42%, and assuming Pfizer was 100% safe for pregnancy (which it’s not) it caused 1.5% of the women who received the Moderna vaccine while pregnant to have a miscarriage. Given that FOIAs showed the V-safe data that was given to the public was cherry picked and highly misleading, and that the Moderna vaccine was given to over 100 million Americans, this quickly adds up. Further, data also shows that global fertility rates have dropped since the mRNA vaccines hit the market and many of us know vaccinated women who are struggling to have a pregnancy.
Note: to illustrate why this is a low estimate, one study found that between weeks 6-11 of pregnancy, less than 1.6% of women suffer miscarriage (while after 11 weeks, the rate becomes far smaller), whereas a 3.3% - 4.8% miscarriage rate was seen in those who received these vaccines.
•Igor also found that of the 12,253 live births in those who received a Pfizer vaccine, 12 infants died (0.09793%), whereas of the 7,916 live births in Moderna recipients, 15 of the infants died (0.18948%), indicating that the Moderna vaccine was 93.48% more likely to cause infant death than Pfizer (a result that again was statistically significant).
•Final Igor found a study that showed that women who took the Moderna vaccine during pregnancy compared to those who took the Pfizer vaccine had a 260% increase in birth defects (many of which were quite severe), a 48% increase in NICU admissions, and a large increase in preterm births (0/42 vs. 4/34).
This data in turn suggests that a dose response relationship exists and that the “longer duration of protection” from Moderna’s vaccine was counterbalanced by a myriad of consequences including aborting a lot of American women (2-3% of pregnancies quickly adds up). What makes this particularly remarkable is that ACIP did not recognize this red flag, despite it being on the slides they publicly presented..
Burying Inconvenient Data
One of greatest frustrations for the vaccine safety movement has been that there has always been an embargo on getting the data which could accurately assess vaccine harm—something typically justified under the logic that the vaccine program is so critical to public safety that it is in everyone’s best interests to avoid giving out data which the anti-vaxxers could then use to create vaccine hesitancy.
For example:
•Patients who got the smallpox vaccine frequently caught smallpox, became severely ill from the vaccine or died. However, doctors covered this up (and were called out in publications of the time for doing this).
•When the infamous 1955 Cutter Incident happened (a hot lot polio vaccine was released onto the market, giving over 220,00 recipients polio), the government chose to ignore its own scientist’s warning (who had found live polio vaccine was present) and instead (like the leaders of the medical profession) continually told everyone that the vaccine was “safe and effective.”
•When the National Vaccine Injury Act (which exempts manufacturers from liability for vaccine injuries) was passed, a key provision of the bill was having a publicly available registry (VAERS) so the public could report vaccine injuries and have access to the accumulated data. That measure was specifically put into the law because the parents of the injured children consistently found that doctors, pharmaceutical companies and Federal health authorities would refuse to document the injuries they reported and then insist that the injuries couldn’t be real because no evidence existed of them happening.
Note: since VAERS was created the government, the medical-industrial complex, and the media have done everything they could to undermine it.
•No publicly available study has ever compared the health of children being given the vaccine schedule to that of children not being given the vaccine schedule, under the argument that “since vaccines are so safe and effective” it’s medical malpractice to deny children life saving vaccines. In turn, when one pediatrician finally did something similar to this (analyzing and publishing the data from his practice—which included many children who were not vaccinated or followed gentler vaccination schedules) and found reducing vaccination immensely improved this health, the Oregon medical board took away his medical license.
•When the CDC conducted a study to disprove the link between vaccines and autism, its raw data showed the opposite. The CDC in turn altered the study to conceal that link—something we found out after one of the lead scientists became a Congressional whistleblower.
•The CDC created a system (the VSD) to monitor vaccine safety, but despite decades of FOIAs, its data has never been made available to the public or independent researchers.
•After an AI system was made for the government to assess the frequency of adverse vaccine effects, it found that 9.4% of vaccine recipients experienced adverse reactions to vaccination but less than 1% of injuries were reported. This in turn led to the system getting scrapped.
•Now that the COVID-19 vaccine injuries are no longer possible to cover up and the federal health authorities have lost the public’s trust, limited apologies are starting to emerge. All of these (e.g., the New York Times' recent plea for vaccine amnesty) typically offer the excuse that the dangers of the COVID-19 vaccines were kept from the public to avoid creating “vaccine hesitancy.”
Despite all of this, determined vaccine safety advocates are nonetheless able to get data comparing the health of vaccinated to unvaccinated individuals. In all cases, these show a massive increase in all the common diseases of childhood (typically at least 2-10 times) that coincidentally have skyrocketed in parallel to more and more vaccines being given to America.
Note: I attempted to compile and summarize that evidence here.
Nonetheless, whenever that evidence is presented, it is typically attacked on the grounds it’s “flawed” or not good enough (e.g., it needs to be from a randomized trial). Understandably, this paradigm is immensely frustrating for vaccine safety activists, as it's clear to them that the evidence of harm is intentionally being withheld to deny any evidence of harm exists.

In my eyes, all of this represents a classic misinterpretation of the principles of evidence based medicine. Specifically, the foundational principle of evidence based medicine is that:
Evidence-based practice (EBP) is the conscientious and judicious use of current best evidence in conjunction with clinical expertise and patient values to guide healthcare decisions.
In turn, while I strongly agree with this sentiment, I simultaneously strongly disagree with how its actually practiced. For example, using “the evidence” to force someone against their will to receive a vaccination is irreconcilable with taking “patient values” into consideration. Likewise, I believe the meaning behind the “current best evidence” has been grossly distorted. Specifically, rather than being taken at face value (that one should use the best available information to guide how one makes medical decisions), it has been redefined to mean “only high quality evidence can be used to make medical decisions.” Because of this, by my interpretation of EBM, the fact that the best available information shows vaccines have serious safety issues takes priority over the fact no (prohibitively expensive) double blind trials have been conducted to assess if that is indeed true and that this should be the scientific consensus until double blind trials (that could provide better evidence) are done to assess the question.
Put differently, since the “best available evidence” shows the vaccines are dangerous, the burden of proof should be on the regulators and pharmaceutical companies to prove their drugs are as safe as claimed—not for them to insist our evidence isn’t good enough while simultaneously withholding the pertinent data and not providing better evidence.
Note: something many do not know is that the Pfizer, Moderna, and AstraZeneca trials were rife with fraud which both the participants (who got severely injured and then kicked to the curb) and the trial investigators repeatedly tried to report to the FDA. However, both the FDA and the medical journals deliberately ignored this—in fact, the FDA got the whistleblower (who I regularly correspond with) fired, and most of the medical community still believes those fraudulent trials are the gold standard of truth for determining if the vaccines are indeed safe.
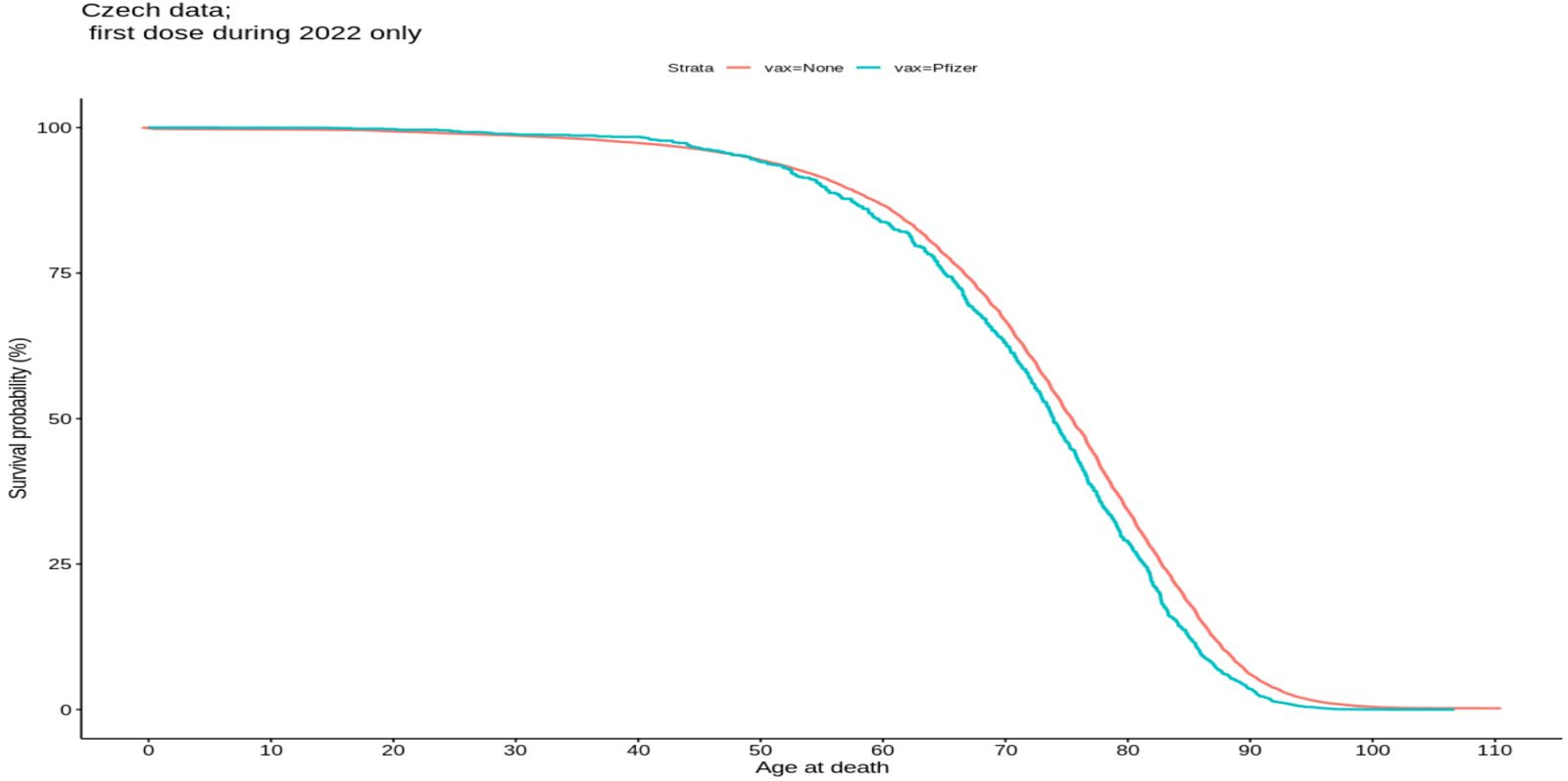
The Czech Data
Due to the existing status quo, for decades it has been immensely challenging for vaccine safety advocates to unearth the actual data on the safety of vaccines. However, since COVID-19, this has changed because so many people have been harmed by the vaccines that a far larger number of people are looking for that data, and far more are willing to leak what the government won’t disclose (or file lawsuits to get it) and far more are interested in it (allowing that data to quickly go viral).
One of the individuals who has been the most dedicated to getting that data has been Steve Kirsch, who has argued that the thing which would definitively settle this is if we could get record level data of large numbers of people showing if they were vaccinated, if they died and how far their death was from vaccination. In contrast, all the data given to us is a carefully curated concoction designed to give the illusion of safety and efficacy (e.g., “95% effective”).
In turn, like each time in the past, a lot of work has been done to maintain the embargo so we can’t actually evaluate how safe the vaccines are. Fortunately, as more and more people are waking up to the dangers of the vaccine, more and more cracks are appearing in the dam, and the truth is gradually starting to pour out (e.g., a data administrator in New Zealand risked his freedom to leak a database that showed the COVID vaccines were killing people and national television stations like this one in Australia are starting to host segments on the dangers of the COVID vaccines).
Recently, a critical crack appeared. Steve Kirsch was able to find record level data from Chezoslovakia of 6,818,692 vaccinated individuals, which was obtained through a FOIA request and was thus authentic. Recognizing the importance of this (as we’ve never had access to a dataset like that before) Steve reached out to a few people who’d helped him on his analyses in the past, and let me dive through it. Like Steve, I believe this is a very important dataset, and this article was essentially written to expand upon some of the points his analysis raised that went beyond the scope of what could fit into the initial analysis.
Steve Kirsh’s full analysis can be read here, a follow up analysis (which took additional factors into consideration) here, and his abridged analysis here.
Pfizer vs. Moderna Mortality
Since that dataset also included which lot the individual had received and their age, a lot of different analyses were possible in it. One of them compared 5,449,549 people who took the Pfizer vaccine to 516,536 who took Moderna’s vaccine. This data found that those who received the Moderna vaccine were on average 30% more likely to die than those who received Pfizer. Furthermore, this difference between Pfizer and Moderna increased as one became younger (e.g., in the 24-34 age brackets, certain ages were 2.1-3.1 times more likely to die and the 20-29 age bracket overall was 2.34 times more likely to die.

Almost every dataset has potential issues which make it questionable. However, since this dataset showed the complete history of an entire population and compared the outcomes of two different mRNA vaccines (which essentially were given to the population in an equally random manner), almost all the potential confounders disappear—especially since regardless of how you analyze it, the 30% increased mortality from the Moderna vaccine relative to Pfizer keeps on coming up. Given that this figure is identical to what all of the previously mentioned analyses concluded, it’s difficult to argue against its authenticity, especially since others have now replicated Steve’s analysis.
Note: Kirsch posted a rebuttal of each attempt to debunk his analysis (that others have now replicated). In my opinion, none of the critiques were able to invalidate Kirsch’s conclusions.
Other Discoveries from the Czech Data
There were also a few other noteworthy things revealed by this data.
Toxicity of the Other Vaccines
One of my big regrets with the COVID vaccine rollout was recommending J&J as the safest option if they absolutely had to vaccinate (which I did not encourage) as half the people I know who then did that had significant side effects from it which resulted in them becoming disabled and not able to work (where the others had no issues). I still believe the long term effects of the J&J vaccine are less than the mRNA ones, but acutely, it seems to cause more problems (e.g., Dennis Rancourt’s meticulous VAERS analysis that found Moderna was 1.3X as toxic as Pfizer also found J&J was 4.0X as toxic as Pfizer). In this analysis, Steve found that the J&J vaccine was actually the most dangerous one (roughly twice as dangerous as Pfizer rather than 1.3 times like Moderna). Curiously, the AstraZeneca vaccine (which has the same design as the J&J one and was notorious for causing deadly blood clots) had a comparative toxicity to Moderna.
Conversely, Novavax (which unlike the other vaccines did not cause the spike protein to be mass produced within the body) had a much lower toxicity and the Pfizer vaccine was a 1.6 to 4.7 more deadly than Novavax’s (however there was much less data available to make this conclusion). That said, the only person I know who waited until the Novavax to take it (so they could work) developed moderate cardiac complications from it.
Vaccine Efficacy
One of the major debates with the COVID vaccines has been whether they reduce your chance of dying (as that’s the only remaining justification for them as every other use such as preventing transmission has now been debunked). Much of this debate essentially boils down to if the hospitalization statistics are being accurately represented (e.g., we’ve established that many vaccinated who get hospitalized are being mislabeled as “unvaccinated”) or adjusting for the fact healthier people are more likely to vaccinate.
This dataset provides another way to evaluate the question. The rationale for Moderna having a higher mRNA dose is that it would be more effective at preventing COVID-19 (e.g., one of the healthcare workers I know who developed permanent complications from Moderna specifically got it because she wanted the higher theoretical protection it afforded). However, in this data, the difference in deaths between Moderna and Pfizer remained the same, regardless of it a COVID wave was happening or when less dangerous variants (e.g., Omicron) were circulating. Given this, it can only mean either that:
•The “protection” the vaccines provided was independent of their dose (which is unlikely given that the Moderna vaccine was shown to generate a much higher antibody response—something expected by their increased mRNA dose).
•The vaccines did not prevent hospitalization and death.
Gender Differences in Mortality:
There was a significantly higher number of men than women who died after receiving the vaccines. This altered mortality ratio in turn suggests that the vaccine is indeed dangerous. I suspect this in part was due to vaccine myocarditis being more likely to affect men.
Note: a 2017 study in Africa conclusively showed that the routine DTwP vaccine (which due to immense public protest was taken off the market in the United States) significantly increased children’s risk of dying by 5 times. However, this risk was different by gender (boys were more 3.98 likely to die whereas girls were 9.98 more likely to die). For those wishing to learn more about the century of evidence clearly linking DTP vaccination to sudden infant deaths, it can be reviewed here.
Co-Morbidities and Mortality
The data also showed that having pre-existing illnesses had no relationship to one’s risk of being killed by a vaccine (which goes hand in hand with the vaccine frequently killing the youngest and healthiest members of society). Like the gender differences these indicate the vaccines have a unique mechanism of toxicity which goes outside of the standard (expected) causes of death.
Timing of Mortality Increase
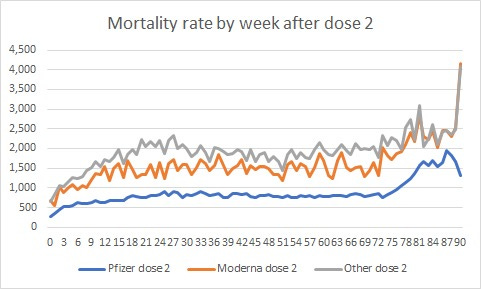
Kirsch showed that there is a steady and consistent rise in mortality risk for roughly 25 weeks after the vaccine is given at which point the risk remains permanently elevated. This is very concerning.
Pfizer Increased Mortality
It was also possible to infer if taking the Pfizer vaccine was more deadly than doing nothing, and once it was found to increase your risk of dying by 34%.
Note: when you put these two figures together, it means receiving Moderna increased an unvaccinated person’s risk of death by 72%.
This in turn is consistent with all the other evidence showing that the vaccines have created an unprecedented spike in death around the globe, especially in younger people who typically do not die. For example, consider how the death rate changed in America’s workers (typically the healthiest members of society) at the time the COVID vaccines were introduced:

Why is The Higher Dose More Toxic?
The fluids of the body depend upon mutual strong negative charges (their zeta potential) to keep this components separate. In turn, when strong positive charges predominate, those components will clump together (e.g., aluminum’s strong positive charge is used to treat sewage by having the suspended organic matter clump together at the bottom of the treatment tank).
This is particularly problematic within the blood as once blood clumps together, microclots form which then block critical circulations within the smallest vessels. Since the brain’s vasculature is particularly vulnerable to this, neurologic injuries frequently follow significant disruptions of the physiologic zeta potential. In turn, one of the biggest problems with vaccines is that they carry a strong positive charge (primarily due to their aluminum component) which causes microstrokes that lead to long term neurologic damage, and can easily be detected with a neurological examination.
Early on, I realized the spike protein (and later the vaccine’s lipid nanoparticles) also carried a strong positive charge which was highly disruptive to the physiologic zeta potential (something which has since been proven). In turn, many of the side effects the COVID vaccines created were similar to what I had seen other vaccines do, but far more frequent and severe in their intensity (e.g., a lot of people I know who took the COVID vaccine no longer have eyes that smoothly track from side to side). Because of this, a central mission of my Substack has been to spread the awareness of the Zeta potential concept, as improving it (discussed here) represents one of the simplest ways to heal vaccine injuries and restore health.
To circle back, a key point discovered by all the pioneers of the zeta potential concept is that each disruption to it is cumulative, and that each individual has a critical threshold they pass at which the body flips over to a micro-clotted state and a variety of injuries emerge. Because of this, higher spike protein doses (e.g., those created by the vaccine rather than a natural infection, or those created with Moderna compared to Pfizer) were more likely to pass this critical microclotting threshold.
Note: sadly this is not the only reason why an excessive dose of the mRNA technology was incredibly dangerous.
Pumping and Dumping
In this publication, I’ve argued that a lot of irrational policies in medicine only make sense if you understand the financial motivations behind them.
For example, in a recent article, I discussed how “pumping and dumping” is a common way the biotech startups monetize the newest pandemic by baiting investors into buying into their miraculous cure for the pandemic and pumping the stock up while the startups dump the shares before they crash—making a great deal of money for the startup by taking it from the investors.
Consider for example Moderna’s stock history which made their CEO be worth over 4 billion dollars.
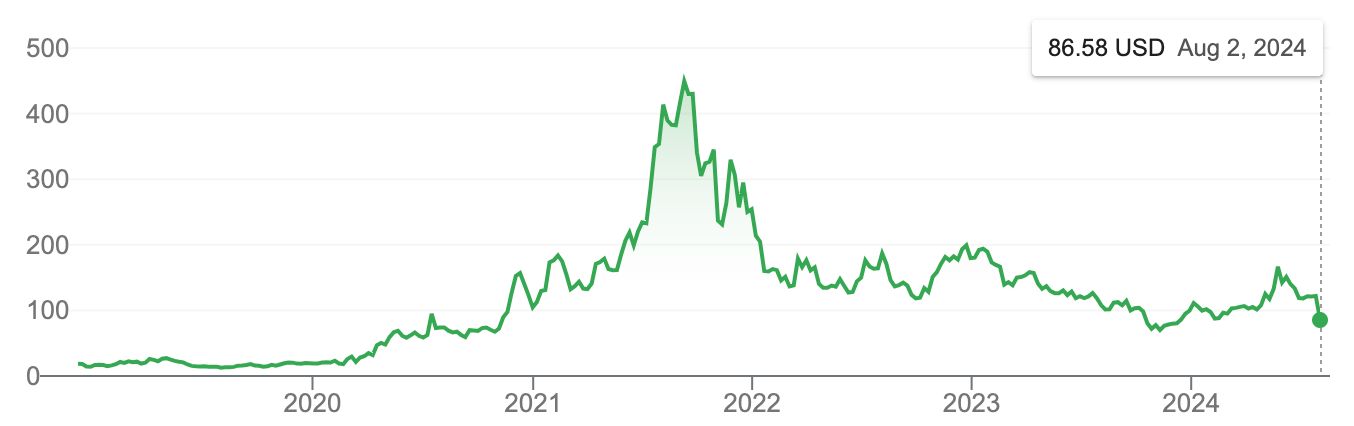
Note: Moderna was private from 2010-2018 and hence did not have a public stock price.
In 2016 and 2017, two remarkable articles were written about the startup Moderna, which was founded in 2010, received more than 2 billion dollars in investments, and conducted numerous pharmaceutical partnerships to create a viable drug but had failed to bring a product to market. These articles predicted much of what happened during COVID-19 and my belief is that if these articles had been read prior to the vaccines coming out, no one would have taken Moderna’s product.
The basic issue Moderna ran into was that there was no way to make an mRNA gene therapy which both was given in a high enough dose to produce a sufficient amount of the target protein (e.g., one missing due to a genetic defect) that simultaneously was not excessively toxic to human beings. For example, Moderna eventually settled on the easiest to treat genetic disorder they could identify (due to it requiring a much lower protein product to be produced in the body) and convinced a large pharmaceutical company to invest 200 million in it, but could not make it safe enough to test in humans and gave up on it.
Every drug has what’s called a therapeutic window..For mRNA, that has proved elusive.
mRNA is a tricky technology. Several major pharmaceutical companies have tried and abandoned the idea, struggling to get mRNA into cells without triggering nasty side effects.
Nonetheless, Moderna was able to attract significant investment through having a CEO (who had no scientific background) who effectively sold the euphoric message to investors that the human genome was like software, and with mRNA technology, the medicine of the future would simply be rewriting the programming code within us.
And so he became the company’s CEO — and soon developed an almost messianic reverence for the mRNA technology.
Because of this, investors continued to support the company despite its lack of a viable product to bring to market (even after it pivoted into the far less lucrative field of mRNA vaccines rather than using it to treat genetic disorders).
Those who buy in are all in: Some employees speak with respect bordering on awe about Moderna’s promise, with one likening the technology to “magic.”
The CEO accomplished this by having a militant culture within the company (characterized as a “caustic work environment”) that fired anyone who did not produce the desired results (e.g., successful experiments) or anyone he felt was not loyal to his ideology.
This, in turn, resulted in a mass exodus of his top talent (which was a red flag to investors) and a rigid culture of secrecy. Moderna refused to publicly publish its data, and everyone involved with the company (even those interviewed) were forced to sign harsh NDAs. In parallel to this, Moderna’s CEO promoted mRNA on CNBC and CNN, taking part in segments on the world’s most disruptive companies and the potential “cure for cancer.”
Bancel (Moderna’s CEO) has repeatedly promised that Moderna’s new therapies will change the world, but the company has refused to publish any data on its mRNA vehicles, sparking skepticism from some scientists and a chiding from the editors of Nature.
In turn, at the time the Stat news article was published, there were signs Moderna’s grift was nearing its end, and hence, the CEO was willing to take a big risk (e.g., using a toxic dose) to save the company.
“[The technology] would have to be a miraculous, Hail Mary sort of save for them to get to where they need to be on their timelines,” one former employee said. “Either [Bancel] is extremely confident that it’s going to work, or he’s getting kind of jittery that with a lack of progress he needs to put something out there.”
Note: the Robber Barons was a 1962 book that chronicled the post Civil War rise of the richest individuals in history (e.g., Rockefeller). Most of these individuals were what the author termed “projectors” who had the ability to create the facade they would be immensely successful and pull many others into their schemes—allowing them to quickly create wealth from nothing, at which point these unscrupulous and daring scoundrels became extremely cutthroat and methodical in doing whatever they could to create their empire and wealth. The key point I took from the 2016 and 2017 articles was that Moderna’s CEO had many characteristics that were identical to the most successful projectors of the previous era..
NIH Royalties
In a recent article, I showed how Anthony Fauci used a recently passed law to transform the Federal scientific apparatus into a pharmaceutical production pipeline by:
•Diverting a large amount of the Federal research budget into projects that could create viable pharmaceutical products.
•Having the commercially viable discoveries be licensed to the pharmaceutical industry to bring to market.
•Paying off the government to approve those discoveries through the promise of royalty payments for their approval to both the scientists who discovered them (who are often connected to the approving regulators) and to the government itself.
•Using the money made from doing this to incentivize more and more corruption within the Federal Bureaucracy until it becomes systemic and a pay-to-play environment is created for drug approvals (e.g., the FDA commissioner who sabotaged hydroxychloroquine being available to the public became the chief medical officer of Moderna’s parent company six months after he left the FDA).
In Moderna’s case, once their gene therapies failed, they switched their focus to the less lucrative field of vaccines and partnered with the NIH. Because of this, shortly after COVID-19 emerged, the NIH’s scientists gave them a genetic sequence to work with to create an antigen to COVID-19 (and thus a vaccine). Following this, the U.S. government gave them 8 billion dollars to develop the vaccine (regardless of whether it was approved) and a liability shield from patent infringement lawsuits.
This was a massive gift, and simultaneously incentivized the government to approve Moderna’s vaccine (due to how much they had to lose if it was not approved). In my opinion, had the government not been financially entangled with Moderna, it’s unlikely its more toxic formulation would have been approved. Likewise, Moderna did not invent any of the key components of its vaccine, but due to the liability shield the government gave Moderna, it was able to claim the final product utilizing those discoveries as its own (and be protected from getting sued for stealing the other company’s intellectual property). Because of all of this, I strongly suspect that had Moderna not had these protections, it would have never brought the vaccine to market.
Remarkably, much of this came to light because Moderna then broke its agreement with the government, refusing to both price the COVID-19 vaccine fairly (rather, Moderna charged an exorbitant price) or pay the royalties it owed the US government for the vaccine. Because of this, the NIH sued Moderna for the lost royalties, and settlements are gradually being reached (e.g., they recently paid the NIH 400 million in overdue royalties for one of the patents in dispute).
In short, Moderna’s CEO deftly maneuvered through both Wall Street and our dysfunctional regulatory apparatus and by doing so was able to get a clearly unsafe product onto the market and ultimately made billions of dollars. Given how disastrous the consequences of this were, I believe it is critical for everyone to understand exactly how we got to this point as that same corruption still exists within the Federal Bureaucracy, and in my opinion, the only thing that can fix is a widespread loss of public trust in the regulatory bodies forces them to address their systemic corruption.
Conclusion
In my opinion, these events clearly demonstrate that the regulators can no longer be relied upon to accurately assess the safety or efficacy of products they approve and that the only path forward is for all pertinent data (rather than just carefully curated journal publications) to be made available so the public can independently investigate it. Sadly, this is not a new issue. For example, consider this 2004 Congressional testimony by the FDA regulator who got Vioxx pulled and exposed the FDA's pay-to-play environment that lets dangerous drugs sail through and never be withdrawn.
I discussed this story with Steve Kirsch while he was working on it (e.g., to share ideas). For this reason, I will quote some of what he published as it encapsulates my feelings on the subject as well:
The regulators didn’t notice such a huge safety signal for Moderna. This opens up the very real possibility that Pfizer is unsafe too and that other vaccines are unsafe as well.
To put it in numbers, if everyone in the US got the initial 2 dose Moderna shot, it would cause a minimum of 650,000 excess deaths (which I estimated at a 20% increase in overall US ACM [all cause mortality] because the ACM rates are much higher for older ages where the % impact of the vaccine is much smaller). That is a conservative estimate. Rancourt et al estimated the COVID shots kill on average for all ages 1.26 people per 1,000 shots. In the US with over 677M shots given, the estimate is over 850,000 deaths.
Even more problematic is that no world health authority, local, national, or international, was able to detect such a massive relative mortality increase of Moderna compared to Pfizer.
The reason is simple: none of them bothered to look.
There isn’t a single mortality comparison by brand posted by a public health agency anywhere in the world ever. Not even in internal documents.
That’s appalling. Yet nobody in the mainstream medical community ever voiced a concern about the lack of this sort of obvious safety monitoring and the total lack of data transparency.
If they looked, they would have found exactly what I found: a major problem. It took me less than 15 hours from the time I got the data to spot the huge anomaly in the data.
This is a major failing of the medical community and regulators. They should all publicly apologize and admit they were inept.
This research has exposed a huge flaw in vaccine safety monitoring. We have to re-examine how so many scientific studies could miss such a huge safety signal and adopt a methodology that reliably reports safety information.
This data means it’s time for the medical community to face reality: they ****** up big time with their willful blindness and 100% trust in the CDC and FDA. Nobody wanted to see any data. Nobody was asking for data transparency.
Bottom line: Keeping record-level public health data secret for all vaccines likely resulted in well over 10M deaths worldwide from these shots. That’s right: governments worldwide killed their own citizens due to their failure to look at the data they collected post-rollout.
In my opinion these events illustrate are a perfect illustration of why the current financial entanglements between the Federal government and the pharmaceutical industry are unacceptable and must end.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.