
New Harvard, Oxford study CLEARLY shows the vaccines cause myo/pericarditis, not the virus
A large study of kids in the UK shows that only vaccinated kids got myocarditis and pericarditis. The numbers are hugely statistically significant. There is <1 chance in a billion this was a mistake.


Executive summary
My misinformation spreader friends and I have always maintained that nearly all the myocarditis cases and deaths are caused by the COVID shots.
Now, a new large study of nearly 1.7M kids, not yet published in the peer-reviewed scientific literature, confirms that. 100% of the myo/pericarditis cases were in kids who were vaccinated. 100%!!!
This was a study done by researchers at Harvard and Oxford.
There were 12 cases in the adolescent vaccinated cohort and 0 in the unvaccinated. Both groups were evenly matched and, for example, had equal rates of COVID infections prior to enrollment and post-enrollment, the unvaccinated had 6,000 more COVID cases than the vaccinated. So if the virus was the major cause, the case counts would be higher in the unvaccinated.
Also, nearly 10% of the 410K adolescents in each adolescent arm got COVID during the 20-week study period, so they can’t argue that there was no COVID during the observation period.
So it was the VACCINE, not the VIRUS.
There is no possible way this can happen if the COVID vaccine wasn’t causing myocarditis and pericarditis (the chances are less than 1 in a billion).
And because this outcome wasn’t the focus of the study, we are much more likely to believe it.
If anyone can explain how this data shows that it is COVID that is primarily causing myo/pericarditis, I’m all ears!
The paper
OpenSAFELY: Effectiveness of COVID-19 vaccination in children and adolescents

There were 1.66M kids in this study; nearly half (49.4% ) were unvaccinated; the rest had one or more doses of the Pfizer COVID vaccine.
Not one unvaccinated child was found to have myocarditis or pericarditis.
On the other hand:
Let’s do the math!
Let’s use the table from the paper (last two rows). Keep in mind, the two cohorts were evenly matched with exactly the same % of prior COVID infections:

The Fisher exact test shows that it is more than 99.9% certain that the myo/pericarditis rates in adolescents are higher in vaccinated kids than unvaccinated kids.
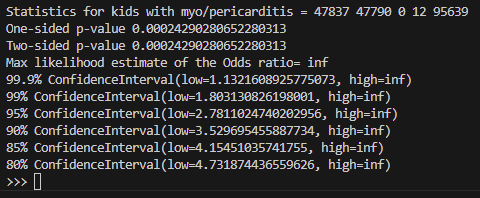
The Poisson distribution also shows this didn’t happen by chance
The chance of seeing 12 events when you were expecting 1 or less is:
8.3e-10
So it’s 1 in a billion for us to see something this lopsided if the vaccine was as safe as claimed.
How do the scientific community explain this? That top UK scientists cannot count?
Nope! It’s that the study wasn’t designed to look at this variable!
But that’s the whole point, isn’t it? If the study was designed to study that variable, then they’d find a way to obscure the signal. Because that is how science works!
The gaslighting explanations
It’s bizarre reading the community notes on this study in a futile attempt to try to convince you that this is not significant. Seriously?
If COVID causes myocarditis, since we all “know” that the unvaccinated get more COVID (because that’s what they tell us), then the unvaccinated should have HUGE rates of myocarditis compared with the vaccinated. But it’s the reverse.
Here’s one of the community notes:
The study looked to understand the "Effectiveness of COVID-19 vaccination in children and adolescents". It was not looking at myocarditis and should not be used as a proof point that vaccines are causal.”
Yeah, that’s right. The study wasn’t about myocarditis, that’s true.
Now suppose everyone in their study who was vaccinated died within 30 days of the shot. This person would caution you that the study wasn’t designed to study that and you should ignore it and get your shot!
What ChatGPT says that the “science” says
The rate of myocarditis after receiving a COVID-19 vaccine is generally lower compared to the rate of myocarditis following a COVID-19 infection itself, particularly in most age groups and across the general population.
Comparison of Myocarditis Rates:
COVID-19 Infection:
The risk of myocarditis is significantly higher after a COVID-19 infection, especially in young males and in adults across a range of ages.
Studies have shown that COVID-19 can cause widespread inflammation affecting the heart.
COVID-19 Vaccination:
Myocarditis following mRNA vaccination (such as Pfizer-BioNTech or Moderna) is rare, and it typically occurs at a higher rate in young males (aged 16-30) after the second dose.
However, the absolute incidence remains relatively low, ranging from 10 to 40 cases per million doses depending on the vaccine and population.
Comparison by Data:
Data from studies conducted in multiple countries show that the risk of myocarditis is around 2-6 times higher following a COVID-19 infection compared to vaccination.
A study from the CDC and data from countries like Israel and the UK indicate that while there is a slight increase in myocarditis risk after vaccination, the risk from infection is substantially greater.
How They Know:
Researchers use population studies that track the incidence of myocarditis in individuals who have received the vaccine versus those who have been infected with COVID-19.
Data sources include national health databases, insurance claim data, and healthcare registries. These studies use statistical methods to adjust for confounding factors and compare rates across different groups.
Agencies like the CDC, European Medicines Agency (EMA), and peer-reviewed journals publish these findings based on observed data across millions of people.
Summary:
The risk of myocarditis is higher following a COVID-19 infection than after vaccination, especially among younger people.
COVID-19 infection raises myocarditis risk by 2-6 times compared to vaccination, depending on the population and vaccine type.
The data is gathered through large-scale epidemiological studies comparing vaccinated versus infected groups across various demographics.
This comparison emphasizes the benefits of vaccination, especially considering the lower overall risk of myocarditis compared to the risk posed by COVID-19 itself.
Let’s compare what the researchers found here
There were 12 cases in 47,800 person-years.
We don’t know how non-linear this is, so let’s assume that it’s linear for the first year.
This means if you gave 50,000 kids the shot and followed them for a year, you’d see around 12 cases. So that’s basically 1 case per 4,000 kids vaccinated based on the study. I think the rate is much higher than that because I know schools with 400 kids where there are multiple cases of myocarditis.
ChatGPT says vaccine induced myocarditis is really rare: around 1 case per 40,000 kids, but the rate of COVID-caused myocarditis is up to 6X higher.
Which is the truth?
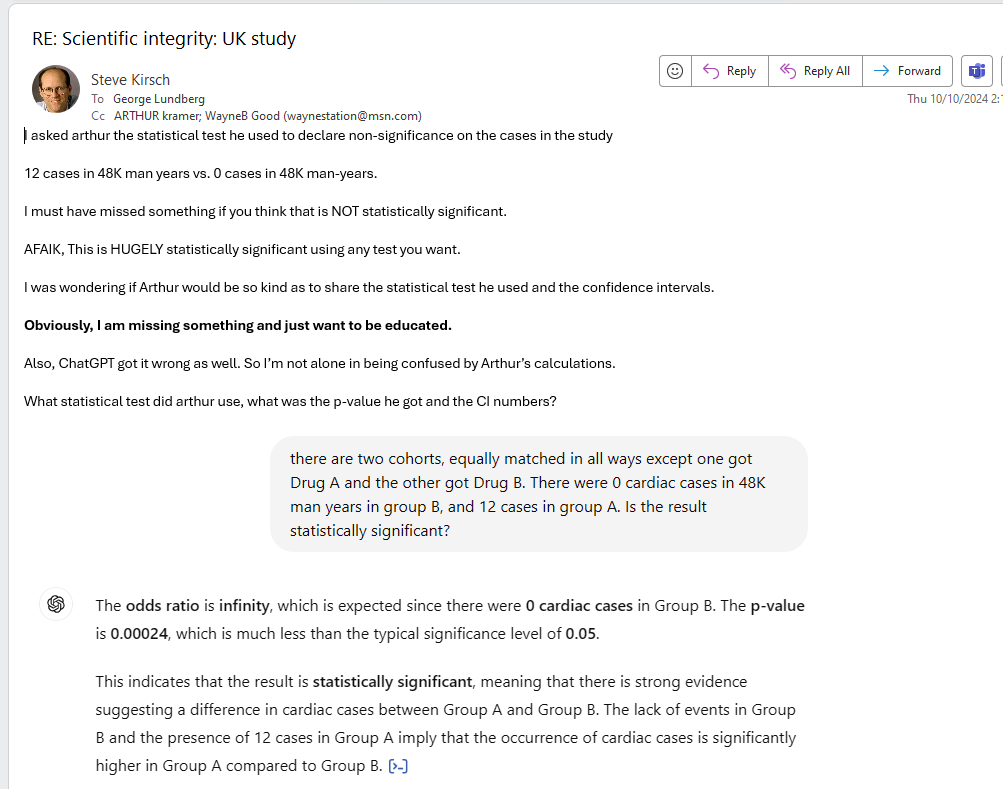
I just sent this email to former JAMA editor George Lundberg and his friends
A large Harvard/Oxford study of nearly 1.7M kids in the UK, which were equally matched in nearly all aspects (including previous covid infections) showed 0 cases of myocarditis and pericarditis in the unvaxxed and a 12 cases in the single vaxxed group.
Here is the chart for adolescents below.
Let’s say that myocarditis and pericarditis aren’t caused by the covid shots.
Then the chance of seeing a result like this is less than 1 in a billion per the Poisson distribution.
So the only viable conclusion is the vaccines are causing myo/pericarditis and COVID is not.
And yet there are many papers showing the opposite and health authorities agree with THOSE papers, not this one.
I was wondering if anyone can explain to me how the Harvard/Oxford researchers got it wrong here.
Thanks!
Replies to my email
An attorney wrote: “If it is 12 cases in 1.7 thousand, that is statistically insignificant. That is 0.7% Would you bet your life on something with less than 1% chance of happening?”
My reply: “Perhaps you can share with me your calculations here including the statistical test you used and the confidence intervals as I am unable to replicate your results. Thank you!”
Then former JAMA editor talked about the rates in other studies without addressing the issue I raised so I repeated my question:
The response they gave me was to avoid answering my question and changing the topic. That’s how it works.
One wrote:
As a physician, not a statistician, I make and act on imperfect information every day.
As a medical editor, I hired biostatisticians to advise on the validity of medical studies.
We all bet odds while making life and professional choices.
I often distinguish between statistically significant and clinically significant; risk vs gain is key; aka cost vs benefit.
If an American male begins to drink alcohol at all, his odds of becoming an alcoholic or problem drinker are about 1 in 15. That Is a serious risk and yet I happily drink wine with dinner. If I knew that the next UAL flight I board has a 1 in 15 chance of crashing, no way would I get on that airplane.
Life's choices.
The other wrote:
I did. You cannot call less than 1% statistically significant. That's elementary school math, which I am sure you mastered at some point.
See why society is in trouble? Nobody is calling these people out on their bullshit.
These results are highly statistically significant and should cause alarm bells to go off.
And yet, nothing happens.
Summary
The medical community will ignore this study, even if it does get published.
But in our view, this study is much closer to the true numbers than what the medical community believes.
Given the lack of consistency in numbers found in the medical literature, if you want to know the truth, your best course of action is to gather your own statistics from your friends, family, news reports, and so on.
Let’s see what my readers think?
Even if there is only 1 case in 50,000 that's still 1 case too many given that the risk of serious harm from Covid itself is virtually nil in kids. I still maintain that forcing this "vaccine" on kids was the most egregiously inhuman part of the entire Covid operation.
Just talked tonight to the owner's wife at a restaurant we patronize and she related that the arm she got the 3 covid vax shots in now trembles and she can no longer carry multiple dishes on that arm. She also related that another customer got Guillain–Barré syndrome after the vax shot and is functionally disabled now. Since we were just informed I thought I would throw that in here tonight.