
Newly Leaked Data Shows Just How Dangerous the COVID Vaccines Are
Why Does the Government Hide Vaccine Injury Data and When Will This Stop?

Throughout my lifetime, I have heard people claim that the future will bring better technology and that science will make the world a better place and solve all our problems. Yet, again and again, these promises fail to materialize, and we are perpetually stuck waiting for science’s promised future.
In many cases however, the technology was in fact developed. The problem however was that the technology’s development threatened someone’s ability to make money (or gain power) so the technology was buried and never saw the light of day. For example, throughout COVID-19 we heard numerous promises that a solution to the pandemic was around the corner (e.g., the miraculous vaccines) yet each time an un-patentable solution (e.g., ivermectin or hydroxychloroquine) was found, the pandemic-industrial-complex ruthless suppressed it to ensure their grift could continue.
Within the field of data, a similar issue exists. The mantra from Silicon Valley which has gradually entered the rest of the culture is that “more data” is the solution to all of our problems. However, once that data gets in the way of someone’s ability to make money, it often never sees the light of day.
In a recent article, I showed how there have been numerous vaccine disasters where a rushed vaccine was developed, the FDA was warned by its own scientists the vaccine was not safe (often due to its rushed production method) and then rather than heed those warnings, the government chose to bring the vaccine to market and have every authority repeat the mantra that the vaccine was “safe and effective.” Then once Americans began to be injected and data started accumulating showing the vaccine was indeed not safe, the government instead chose to double-down on its position, insisting the vaccine was safe and doing whatever it could to cover up that inconvenient data—all of which also happened with the COVID-19 vaccines.
In each of the past vaccine disasters, the dangers of the vaccine were eventually exposed by the media, before long the unsafe vaccine was pulled from the market, and ultimately, there was some degree of accountability (e.g., the responsible officials had to resign or the victims received financial compensation through the courts).
Seeing that this was not good for business, the vaccine industry in turn adopted a few strategies which radically tilted the deck in their favor:
•Bill Clinton in 1997 legalized direct to consumer pharmaceutical (drug) advertisement (something only otherwise legal in New Zealand). Since most of the pharmaceutical industry’s expenditures are in advertising, this allowed them to become the dominant advertisers on television, and within a few years, the networks stopped being willing to air stories critical of vaccinations, even when the CEO personally supported the story being aired.
Note: the final unsafe vaccine the American media exposed was George W. Bush’s 2002 “emergency” smallpox vaccine (which rapidly ended the program because there were too many injuries in the military). Not long after, in 2006, the incredibly dangerous HPV vaccine entered the market, and despite a deluge of injuries, the American media would not touch it—instead it was exposed by a Danish network in 2015.
•Vaccine manufacturers were exempted from liability for their products—instead vaccine injuries were delegated to a federal compensation program which only allowed a narrow range of injuries to receive compensation. This understandably took away the industry’s motivation to produce safer vaccines.
•The vaccine industry worked with the FDA to create a variety of regulations for “emergency” vaccines which waived both the existing requirements to prove safety or efficacy and the ability to pursue the manufacturers in the legal system (either by directly suing them or though the federal vaccine injury compensation program).
Note: the “compensation” program for the COVID vaccines, according to a 2/21/23 congressional report has thus far not provided compensation to anyone injured by these “emergency” products.
The Vaccine Adverse Event Reporting System
In 1986, an Act was passed by Congress to address the growing problem of vaccine injuries. Many remember this act because it gave legal immunity to the manufacturers through the federal compensation program. However, what’s less appreciated about it is that the activists also were able to force two other provisions into it.
First the Secretary of the Department of Health and Human Services was to appoint a Director and a National Vaccine Advisory Committee that would guide the federal agencies to:
Develop the techniques needed to produce safe and effective vaccines.
Coordinate and provide direction for safety and efficacy testing of vaccines.
Promote the development of childhood vaccines that result in fewer and less serious adverse reactions than those vaccines on the market [in 1986].
Make or assure improvements in…the licensing, manufacturing, processing, testing, labeling, warning, use instructions, distribution, storage, administration, field surveillance, adverse reaction reporting, and recall of reactogenic lots or batches, of vaccines, and research on vaccines, in order to reduce the risks of adverse reactions to vaccines.
Note: this has been a longstanding problem with vaccines—hence why the activists insisted something would be done about the hot-lot issue (as the DPT makers did not want to spend a bit more on manufacturing so hot-lots didn’t get out to the public).
Additionally, the Secretary was expected to:
Within 2 years [of 1986] and periodically thereafter, the Secretary shall prepare and transmit to the Committee on Energy and Commerce of the House of Representatives and the Committee on Labor and Human Resources of the Senate a report describing the actions taken [to make safer vaccines].
Within 3 years [of 1986] complete a review of all relevant medical and scientific information [including the research mentioned above] on the link between DPT [and MMR] vaccination and the following conditions…”
Note: Once this report was completed, the secretary was to submit it to Congress, make it publicly available it and modify the vaccine injury table so those conditions would also be covered by the national vaccine injury compensation program, and then repeat this process at least once every 3 years.
The vaccine industry really did not want to do this, so except for DPT (where outside pressures forced them to), those safer vaccines never got made. In turn, the federal bureaucracy [e.g., the FDA and CDC] got around this law by simply choosing to be non-compliant—something RFK Jr. and Aaron Siri finally proved in 2014 when the H.H.S. admitted in court it had not done much of what the act required.
Note: Since 1986, very few conditions have been added to the table of vaccine injuries that will be covered. For reference, those injuries are: rapid-onset chronic arthritis, thrombocytopenic purpura specific autoimmune disorders and catching measles from the MMR vaccine, intussusception from the rotavirus vaccine, and Guillain-Barré Syndrome from the flu vaccine.
Second, it became mandatory to report vaccine injuries (although in practice this happens less than 10% of the time) and for those reports:
…all information reported under this section shall be available to the public.
Note: an exception was made for personally identifying medical information.
This gave birth to VAERS, the system we now use to report adverse reactions to vaccines and independent researchers around the world in turn use to assess the safety of various vaccines.
This provision was put in because those early vaccine safety activists had over and over run into the same problem we still face now—doctors and vaccine manufacturers refused to report the injury (to avoid liability) and the government refused to share any of the information it had demonstrating vaccines were unsafe, which in turn was used to argue there was “no evidence” vaccines were unsafe.
Once VAERS broke their information blockade, the government then switched to doing everything it could to undermine the system, such as:
•Continually attacking its credibility and reliability (and likewise having the scientific establishment fail to do the same).
•Refusing to fix it when solutions were proposed (e.g., in 2010, an AI system was created that detected far more vaccine injuries and concluded VAERS was only identifying 1% of those that were occurring—as you might expect, that system was never adopted).
•Failing to hire the staff needed to run it. This in turn, became a huge problem once the COVID vaccines entered the market (as we went from 50,000 reported injuries a year—which the staff at VAERS could not handle to over 1.7 million from the COVID vaccines). In turn, as a recent investigation from a premier medical journal showed, VAERS has not received the staff it needed to process those injuries and has abjectly failed to fulfill its responsibility throughout COVID-19.
Note: at the time the COVID vaccines got an emergency use authorization, on a now deleted page [archived here], when explaining how vaccine safety would be monitored, the FDA stated that the U.S. government “has a well-established post-authorization/post-approval vaccine safety monitoring infrastructure that has been scaled up to meet the needs of a large-scale COVID-19 vaccination program,” and specifically listed VAERS as part of that infrastructure.
V-Safe
Since VAERS had many alleged shortcomings (e.g., you had no idea how many people were being sampled by it and you had no idea if the reports were being legitimate), a new system was created for the COVID-19 vaccines to effectively evaluate if they were indeed “safe and effective.”
However, before long, vaccine safety advocates noticed two major issues.
First, it was not possible to easily input many of the injuries into V-Safe that were commonly occurring after the COVID-19 vaccines.
Second, the public was not given access to the raw data. Instead, we were given curated assessments of the data from “trusted” experts, who not surprisingly, concluded the V-Safe data showed the COVID vaccines were safe.
Fortunately, ICAN was familiar with these tactics and after 463 days of work defeated the CDC in the courts with an appropriately drafted FOIA request. From that data, ICAN discovered that those “trusted” experts lied and V-Safe actually showed numerous red flags with the COVID-19 vaccines (although much of the V-Safe data sadly has still not been made available).
Note: a similar issue exists throughout the pharmaceutical industry as it will repeatedly conduct trials that show their drug or vaccine is quite dangerous, and then concoct a way to hide those dangers from the final trial report. The industry is able to get away with this because neither the government nor medical profession (both of whom are often taking money from the industry) calls out that behavior and because Big Pharma has successfully lobbied for its trial data to be deemed proprietary and thus permissible to withhold from the public.
Burying Inconvenient Data
In short, as I tried to demonstrate here, and in the first, second and third part of this series, the government has proven time and time again that it will bury data that indicates a vaccine is dangerous or makes the public doubt its declarations that all vaccines are “safe and effective.” This in effect shows why “more data” is not our salvation as we will only be fed a curated picture of it that shows what the establishment wants us to see—rather than an inconvenient truth which requires us to fix an existing problem and actually make the world a better place.
Note: the one place where data has “made things better” is in marketing—as in that industry, there is a financial incentive to have accurate data as that is needed to maximize sales.
So throughout COVID-19, since the government deliberately withheld almost all the data that the COVID vaccines are harmful, we in turn instead have had to use the following data sources:
•Anecdotal ones (e.g., this Substack started almost two years ago after I decided to publish a log of all the injuries occurring within my personal circle, which included 45 fatal or likely to be fatal vaccine injuries). These reports tend be reflexively dismissed as “not being credible” but since they are so frequent and so many are seeing them, it has not been possible to gaslight the population into believing they just “random coincidences” (especially since the sudden cardiac deaths in the young was is so unmistakably unusual).
Note: large polls have likewise shown this. One for example found almost half of Americans believed they were suffering from side effects of the vaccine (with 7% characterizing them as “major”), another found half of Americans believed the vaccines were killing people, and a recent one found a quarter of Americans knew someone they believe had been killed by the vaccine.
•Data from clinical trials. Since it is often quite difficult to clearly untangle what a pharmaceutical does once it gets into the market (as so many other variables get added to the picture), the general consensus is that the risks and benefits of it need to be determined in the controlled environment of a clinical trial. Unfortunately, as there is often so much money on the line, pharmaceutical companies will inevitably rig their trials to favor of their drug (which is why truly independent studies consistently paint a quite a different picture of each drug). In the case of the COVID vaccines, not only were the trials clearly deceptive but numerous whistleblowers came forward testifying as such. Sadly, their testimonies were almost completely ignored.
Note: despite all of this, the data on the COVID-19 vaccines was still bad enough that the published data made it clear the vaccines were not safe. This is largely because the one thing which is very difficult to hide (e.g., by reclassifying the event) in a clinical trial is how many people in each group died. As a result, I typically consider the primary metric to judge a trial by its effect on overall mortality.
•Population wide datasets showing a massive increase in deaths and disabilities. Since COVID occurred throughout 2020, whereas the vaccines were introduced at the start of 2021, those datasets frequently make it quite easy to identify the impact of the vaccines.
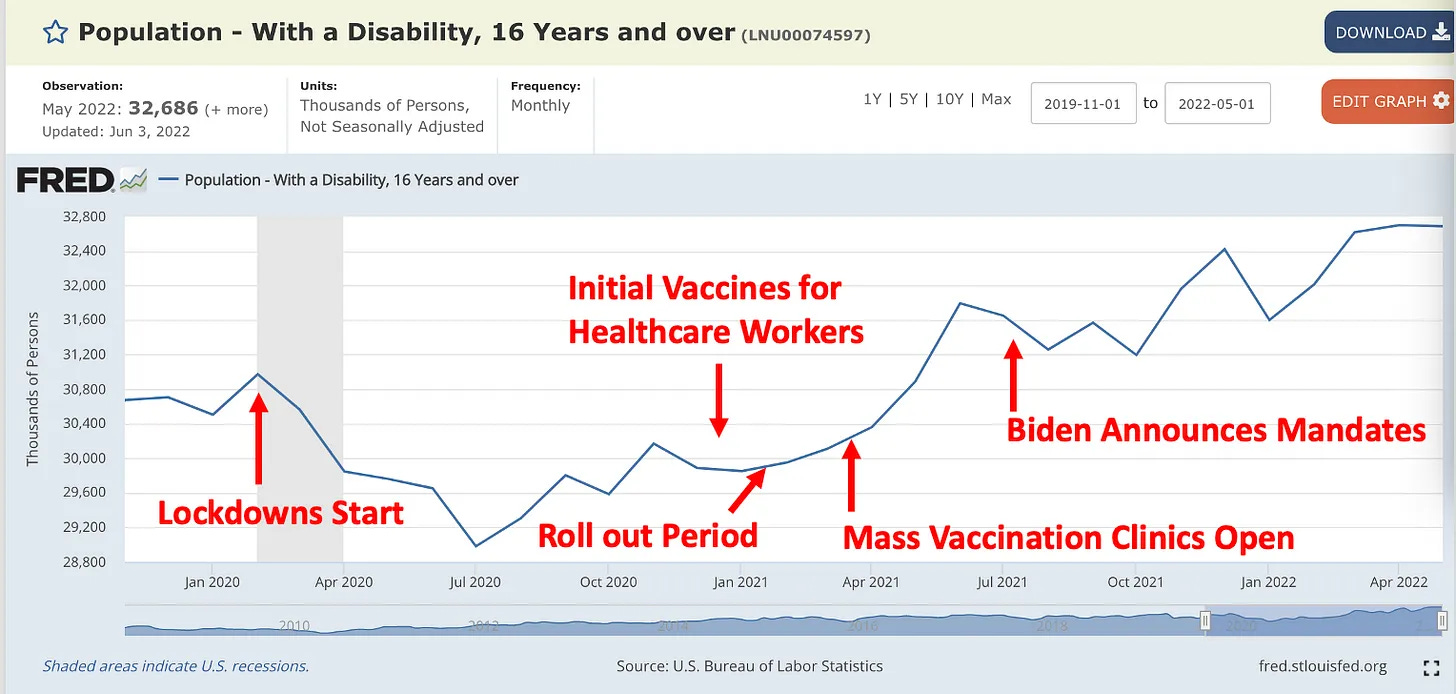
Note: Ed Dowd’s team has done an excellent job of compiling this data, showing the immense cost it has had for our economy and demonstrating that it is statistically impossible it could have happened by chance.
•Data the government withheld that was obtained through lawsuits. The previously mentioned CDC V-Safe data is one example. Likewise, the documents Pfizer submitted for their FDA approval which ICAN also obtained through the courts is another example.
Note: The “FDA approved” vaccine (Comirnaty by Pfizer) was never actually brought to the market. This was done so it could be claimed the COVID-19 vaccine was “FDA approved” (and thus possible for various groups to mandate), but simultaneously, for the dangerous vaccine to retain the blanket liability shield its Emergency Use Authorization provides (hence you can only obtain the EUA but not FDA approved Pfizer vaccine). In essence, we have a situation analogous to Schrödinger's cat.
•Data leaked by whistleblowers. Since the government never will voluntarily disclose data which makes it look bad, data that can only be obtained through leakers inevitably is quite concerning. Similarly, whenever data of this type is requested, the government will always find ways make an unlimited number of excuses to not release that data (e.g., it doesn’t have it or releasing it would violate patient privacy).
Medicare Data
Steve Kirsch has been leading the charge to get the data which will objectively show how safe and effectives the vaccines actually are. Since he has reliably published that information and protected his sources, numerous whistleblowers have contacted him and shared data they risked their livelihoods to obtain.
One of Kirsch’s fundamental principles has been that record level data (raw data) that combines vaccination status with mortality is needed for the world to assess if the vaccines are saving lives or killing people.
Since Medicare has one of the most comprehensive data sources to answer that question (as Medicare tracks when each member is vaccinated and when they die), Kirsch has been working diligently to get that data. Likewise, Medicare was cited by the FDA in the same way VAERS was—as a way to monitor the safety and efficacy of the vaccines.
Note: all the graphs that follow were produced by Steve Kirsch).
First, let’s first look at a typical vaccine:

While it’s not entirely safe (e.g., I’ve admitted an elderly patient to the hospital who suffered a zeta potential collapse from the pneumococcal vaccine), the pneumococcal vaccine is fairly unlikely to kill you, and has a small chance of saving your life from pneumococcal pneumonia. Rather, most of the issues it creates are chronic in nature and take more time to show up.
In turn, if we look at the graph, we notice a few things.
First, there is a drop the risk of dying (mortality) immediately after receiving the vaccine. This is a result of the “Healthy Vaccine Effect” which highlights that sick people at risk of dying are less likely to be vaccinated, and for this reason, the brief initial drop in each graph needs to ignored.
Note: the one spike at the very start most likely represents the small portion of patients who have a severe and immediate reaction to the vaccine like the patient I discussed above.
Secondly, the overall risk of dying stays steady after receiving the vaccine, and if anything is slightly reduced (which I believe comes from the vaccine actually doing what is supposed to do).
In short, the above graph is representative of a relatively safe vaccine.
Next, lets go to the flu shot, a vaccine I consider to be more problematic and likely to injure you (e.g., I’ve run into far more cases of significant injuries following the flu vaccine):
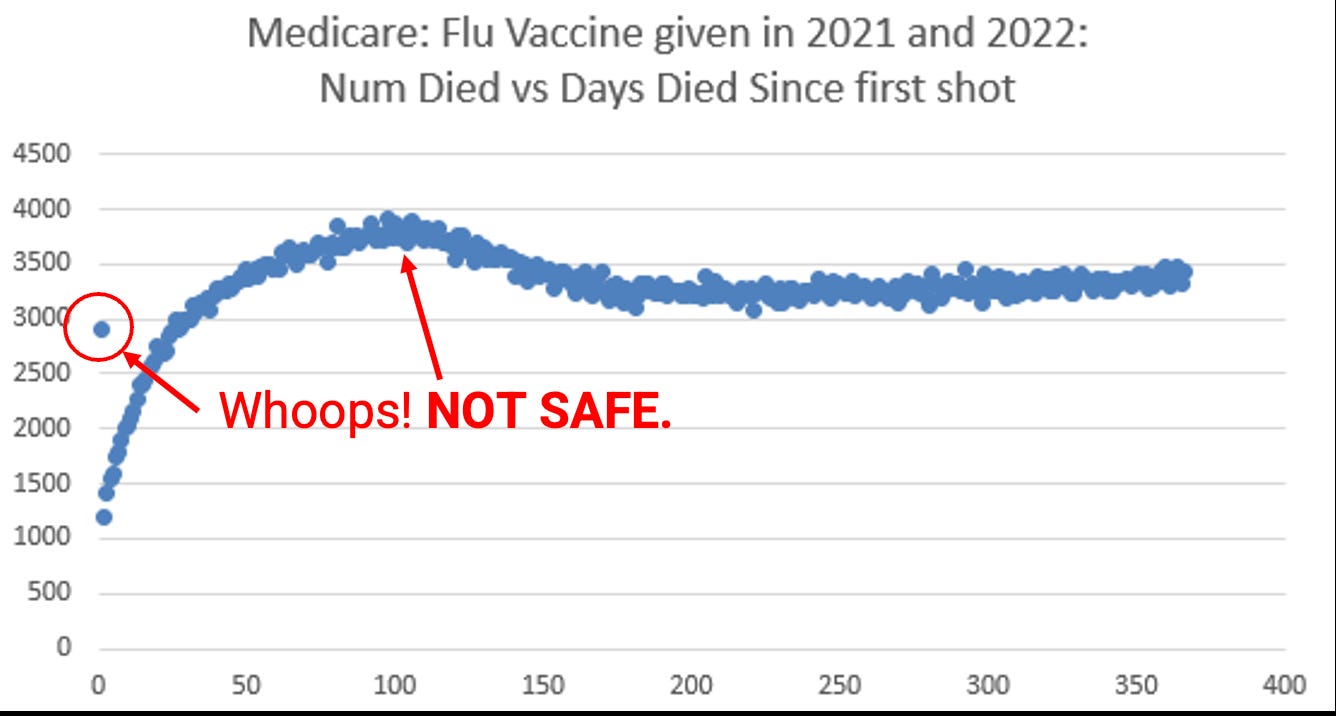
As you can see, there is a distinct spike (roughly 15%) in death following vaccination before the death rate returns to baseline.
Now let’s look at what happens with the COVID-19 vaccines:

Here we instead have a spike that never regresses and instead continues increasing to 30% above baseline. What that seems a bit abstract, it’s a huge deal and provides a concise way to quantify the wave of death we are seeing around us.
Note: given that that same trend is not seen in the flu or pneuomcoccal vaccines which were given in the same time period, it is difficult to argue anything besides the COVID-19 vaccine could be causing it.
Let’s next look at the death trends from one, two and three COVID vaccines.
Note: the drop off at the end is likely due to the data series being incomplete.



Let’s quickly put all of that together into a chart Steve notated:

New Zealand’s Data
Recently, an insider at New Zealand’s ministry of health provided Steve with records tagged to the individual’s age, time of vaccination, number of vaccinations, and date of death (if applicable). This was extremely useful for untangling what is going on, particularly given that New Zealand has a relative small population (5.2 million people) and is known for having relatively good record keeping.
This data set comprised 4,193,438 vaccination records (approximately 12 million COVID vaccinations have been administered in New Zealand), and was composed of 2,215,730 unique individuals (37,285 of whom died). So in essence, it covered a third of the vaccinations and slightly over half of the population. Let’s see what it found:

This graph again shows that the COVID vaccine dramatically increases your risk of dying (Mortality Risk or “MR”), and sadly, that this effect persists for months afterwards.
Likewise, that risk increases as you get more of the vaccines.

This is important because it is both consistent with what we’ve seen throughout the vaccination campaign (the vaccine toxicity increases with each successive dose) and the general laws of toxicology (more doses of a toxin are more likely to kill someone).
The next chart is what I consider to be one of the saddest ones:

Throughout my medical career, I have heard a few stories I could never confirm (e.g., from a nurse who had worked at a facility years ago) of an influenza vaccination campaign being followed by a significant number of deaths in the nursing home. The best explanation I was able to come up with for those events was that the elderly tend to have a poorer physiologic zeta potential (due to declining kidney function) and as a result, they are much less able to tolerate the additional impairment in zeta potential that either an infection (e.g., the flu) or a vaccine can create.
However, while I believed this was an issue, the effects I observed were less overt (e.g., the progressive cognitive decline following the vaccine) rather than overt and life-threatening (e.g., while it happened, it was quite rare I admitted someone to the hospital for a vaccine injury in the pre-COVID vaccine era).
Note: Suzanne Humphries MD, a nephrologist who has done a great deal of important work exposing the dangers of vaccines said her work in this field was started her observation the flu shot would frequently precipitate a kidney injury that required hospitalization or worsen it in a patient who had already been hospitalized for one.
Once the COVID-19 vaccines hit the market, one of the most common stories I heard was an elderly patient who had rapid cognitive decline after the vaccine and then died shortly afterwards. In each case, while the relative was certain it was caused by the vaccine, the death was written off as “Alzheimer’s” or “old age.” I, in turn, believe much of this resulted from these vaccines being much more toxic than the typical vaccine (e.g., they had a much larger effect on the physiologic zeta potential).
This wave of injuries was particularly depressing to watch, because even when large clusters of deaths occurred at a nursing home following the vaccination no one seemed to want to acknowledge this was a problem and reconsider the vaccinations. Rather, before long, the residents often got boosted.
Note: in addition to numerous examples where this was documented, I know of one worker who witnessed it first hand at their facility but had no avenues to report what he was seeing.
Remarkably enough, in medicine, one of the central dogmas when caring for the elderly is that they are “vulnerable” patients who need to be protected since they often lack the ability to advocate for themselves. While I completely agree with this (you see many sad cases of the elderly being taken advantage of because they cannot protect themselves), that dogma goes out the window for vaccines because of the widespread belief they are “100% safe and effective.” In turn, the medical field believes the elderly should always be vaccinated as much as possible regardless of the injuries that occur from doing so or how unclear their consent was to being vaccinated in the first place.
Note: one of the most important things to appreciate about this data is that the deaths are only the tip of the iceberg, and for each death, there are a significantly greater number of chronic and debilitating injuries (e.g., Dowd’s team found there were 10-20 times as many disabilities as deaths).
Replicating the Data
Many of the physician authors I believe have done the best job illustrating the crimes of the pharmaceutical industry have had a common mantra—the data for the drugs we consume must be made public. Yet, over and over this never happens, and those authors in turn are able to show the catastrophic harm that occurs from the data being kept secret.
Conversely, Kirsh’s aim has been to make all the data he has collected be available to the public so everyone can access it and verify his claims (which can be accessed here).
Note: Datasets from a variety of sources are posted in the Wasabi folders. With the spreadsheets containing the NZ data, each column was randomized so that the statistics of the dataset would be maintained, but personally identifying information would not be.
In turn, before publishing this, I attempted to see if I could replicate Kirsch’s findings and see what else I could find within the dataset. Since many graphs have been produced showing an increase in mortality following the vaccine rollout, I decided to see how the deaths in the vaccinated would compare to the total deaths in the population. To create this sheet, in addition to Kirsch’s data, I also utilized Google’s dataset of how many people had received at least one dose, and New Zealand’s monthly death rates (e.g., this one).

Note: if you use the randomized data Steve has provided to create this chart, the sheet you will produce will be very similar but slightly different from this one. Additionally, the peak in deaths is more pronounced if you were to instead make this chart with the elderly.
What all of this data (and others like countless VAERS analyses) have shown is that the COVID vaccines have killed millions of people, and that the majority of those deaths occur months after the shot and predominantly affect the elderly.
If you have a background in data analysis, I would strongly advise you try to look at the data as well, both to confirm for yourself the vaccines are indeed harmful and to see what else you can find in the dataset.
New Zealand’s Data Analyst Goes Public
On November 28th, the chief data analyst for New Zealand (and the source of the above data) decided to go public and disclose what he was uniquely positioned to observe with the vaccination roll-out. Specifically, he found that there was a massive spike in deaths immediately following the vaccines being deployed. Furthermore, he also shared that in a few instances, hot lots were being given that killed between 4.5-21.3% of the recipients and that a few vaccinators had between a 10-24% death rate in those they vaccinated, but for some reason did not speak up. His entire presentation can be seen in the video below and helps put into words what it is like to be shouldered with the responsibility he had (while everyone else was staying silent).
Conclusion
Ever since I first saw how over the top the efforts were to sell the COVID vaccines, my belief has been that marketing and sales would predict everything which would happen with them. More specifically, each time a market was capped, the rules would be changed so a new market could be opened up. To illustrate:
•Initially the vaccines were sold under a scarcity model to get as many people as possible to receive them.
•Once the scarcity model stopped working, they were traditionally marketed to the population.
•Once that market was capped, bribes (e.g., gift cards) were given to incentivize more people to vaccinate.
Note: many of those bribes were so ridiculous (e.g., drugs, donuts and sex) they made many realize there had to be something wrong with the vaccines.
•Once that market was capped soft mandates (e.g., to travel or go to a bar or to a concert) were implemented.
•Once that market was capped, hard mandates were implemented (e.g., losing your job or being kicked out of your educational program).
•Once that market was capped, they started pushing the vaccine on children.
•Once that market was capped, they decided the vaccine actually didn’t fully protect you and boosters were needed.
•Once that market was capped, they decided more boosters were needed and eventually that the vaccine would instead become an annual shot.
As I watched this predictable chain of events, I also told many people that once it was clear the vaccines could not be sold anymore, they would begin acknowledging the injuries were real (e.g., Yale recently published a paper on “Post Vaccination Syndrome” which will likely be shared throughout the medical community). This would of course be done so they could pivot to selling proprietary pharmaceutical drugs that could be used to treat the vaccine injuries.
Note: I suspect this new wave of therapeutics will also include monoclonal antibodies to the original spike protein (which Biden took off the market) and complement factor B inhibitors, new anticoagulants and the existing (but expensive) intravenous immunoglobulin therapy.
At this point, all of us believe the healthcare authorities are fully aware of the current disaster and are doing everything they can to cover it up. In turn, we expect a few people will be thrown under the bus to protect the industry so business can essentially continue as usual. I believe things are very close to a tipping point now because:
•The majority of the population knows the vaccines are not safe or effective.
•More evidence (and leaks) keeps on emerging of the vaccine’s harm.
•There is no longer a financial incentive to cover that up and the funding to keep pushing for them to be on the market (since no one will buy them). Rather the incentive is now to pivot to the even more profitable treatment of them.
Getting to this point we are now has taken a lot of work from many dedicated activists, and I want to sincerely thank Steve for the work he’s put into gathering this data. After he informed me of what he was putting together, I realized the importance of it and hence spent the last two weeks compiling this series which could put those leaks into context. I hope it was helpful for each of you and provided a human face to the immense amount of human suffering which is encapsulated within the abstract data points presented in this article.