
If the COVID vaccine benefit was so large, why can't we detect it in the Czech record level data?
The % rise in all-cause mortality for vaccinated vs unvaccinated during COVID waves were comparable. In other words, the vaccines didn't work.

Executive summary
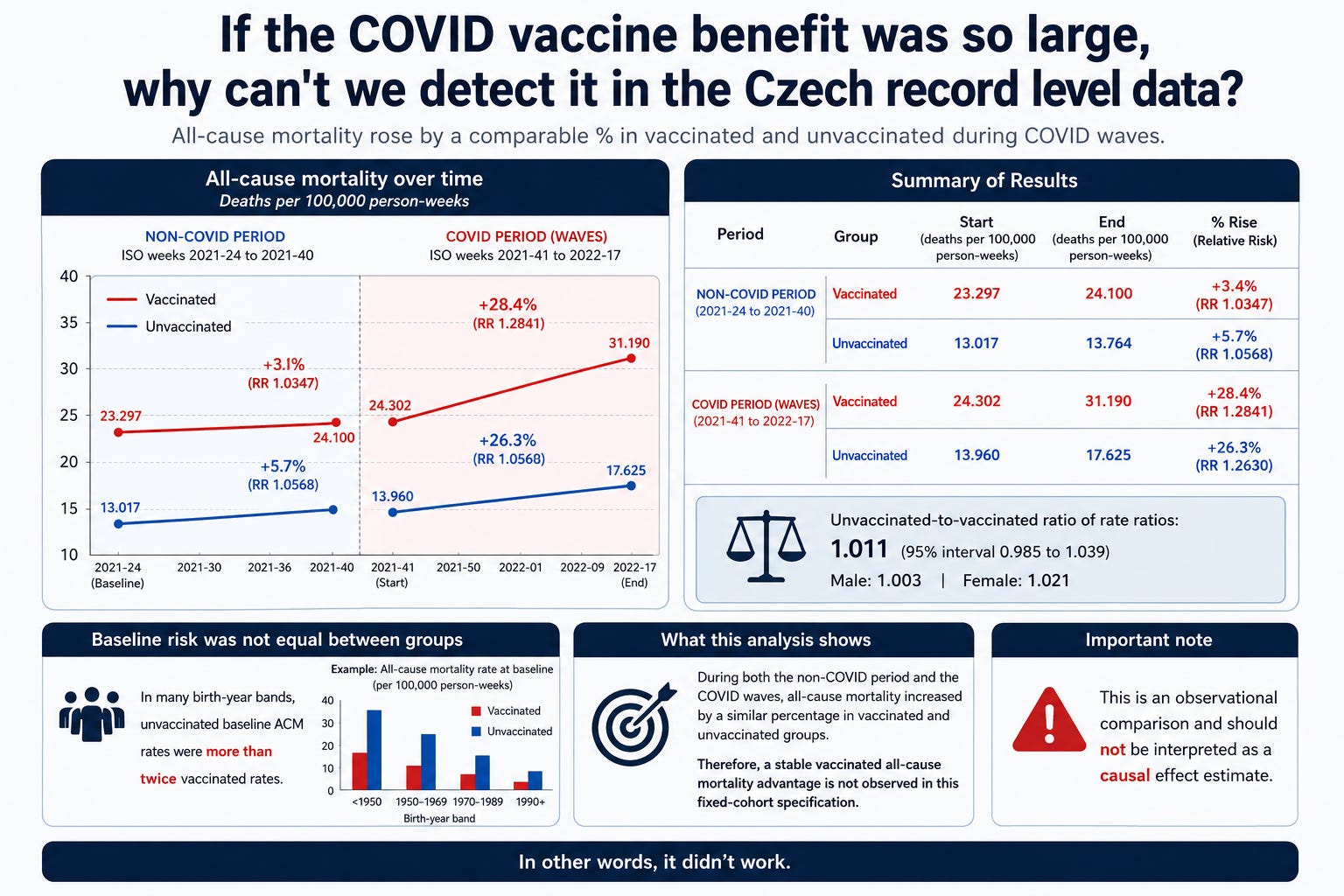
In a fixed-cohort analysis anchored to ISO week 2021-24 (baseline window 2021-24 to 2021-40), vaccinated all-cause mortality rose from 23.297 to 31.190 deaths per 100,000 person-weeks (RR 1.3388, +33.9%), while unvaccinated mortality rose from 13.017 to 17.625 (RR 1.3541, +35.4%). The unvaccinated-to-vaccinated ratio of rate ratios was 1.011 (95% interval 0.985 to 1.039), with male (1.003) and female (1.021) values also close to parity. The two groups did not have equal baseline risk: in many birth-year bands, unvaccinated baseline ACM rates were more than twice vaccinated rates. Nonetheless, the wave-period rise, expressed relative to each cohort’s own baseline, remained near parity, so a stable vaccinated all-cause mortality advantage is not observed in this fixed-cohort specification. This is an observational comparison and should not be interpreted as a causal effect estimate.
In other words, it didn’t work.
My open offer
If you think my analysis methodology of the Czech data using ACM differential cohort mortality during COVID v non-COVID is wrong, then please post the correct method and what it shows. The Czech data has been publicly available for nearly 2 years. If I’m wrong, why hasn’t anyone posted the proper analysis of the data showing a benefit?
I even applied the method used in Palinkas to the Czech data and the results were virtually identical to the method I used.
Pálinkás used regression-adjusted epidemic-vs-nonepidemic HR ratios.
We used fixed cohorts, person-weeks, and all-cause wave/baseline mortality ratio
So two completely different methods, same result. No discernable benefit.
Background
Reliable observational studies comparing vaccinated to unvaccinated are hard to do for a myriad of reasons including:
massive health difference between people who opt to get the vaccine vs. those who don’t (up to 5x mortality rate differences caused by selection bias alone, e.g., Mirror paper)
large differences in testing requirements (required vs. optional)
suppression of symptoms by those who opted for the vaccine leading to under diagnosis.
A lot of people, especially doctors, think that the 5x lower all-cause mortality was due to the vaccine. Nope. We know that for 2 reasons:
When the vaccine rolled out, the population ACM didn’t drop!
And we can measure the mortality difference in the cohorts AFTER vaccination and BEFORE the COVID wave hit. That’s how we know that the mortality differences (which are typically 2x) are due to selection bias, not the vaccine (which only provides a mortality benefit during COVID).
If you look at COVID mortality, it looks like being vaccinated was hugely beneficial. But was that due to these biases?
If we want to know the truth about what happened (instead of feeding our own belief systems), it’s important to look at measurements, such as relative all-cause mortality increases during COVID waves, that aren’t subject to these biases. Other good measurements are following a population (vaccinated AND unvaccinated) longitudinally over time to see what happens (that neutralizes selection biases).
When we do that, we find there wasn’t a clear all-cause mortality benefit at all from those who opted for the vaccine.
In short, we have a vaccine where the best pieces of evidence we have available show significant harm and little to no benefit.
Here are a few examples:
No COVID death benefit: The Medicare US Nursing home data shows the case fatality rate (CFR) remained flat during alpha, even though nursing homes were the first to get the shots. This was literally the “poster child” case study and the CFR didn’t budge directionally. The Arbel study done in Israel claiming the boosters had a 90% reduction in death was later found to be caused by the healthy vaccine effect which nullified the finding (Hoeg).
Increased risk of all-cause death: The Florida brand comparison study by Levi and Ladapo showed even when you closely matched both Pfizer and Moderna groups, those with a Pfizer vaccine had 37% higher non-COVID all cause mortality which is highly suggestive of huge vaccine harm.
Increased risk of cases: Multiple Cleveland Clinic studies pointed out more vaccines—>greater risk of infection. And Israel is the stunning example of that with the highest cases of Delta and Omicron in the world, over 10x higher than their alpha infections which was confirmed by careful wastewater measurements.
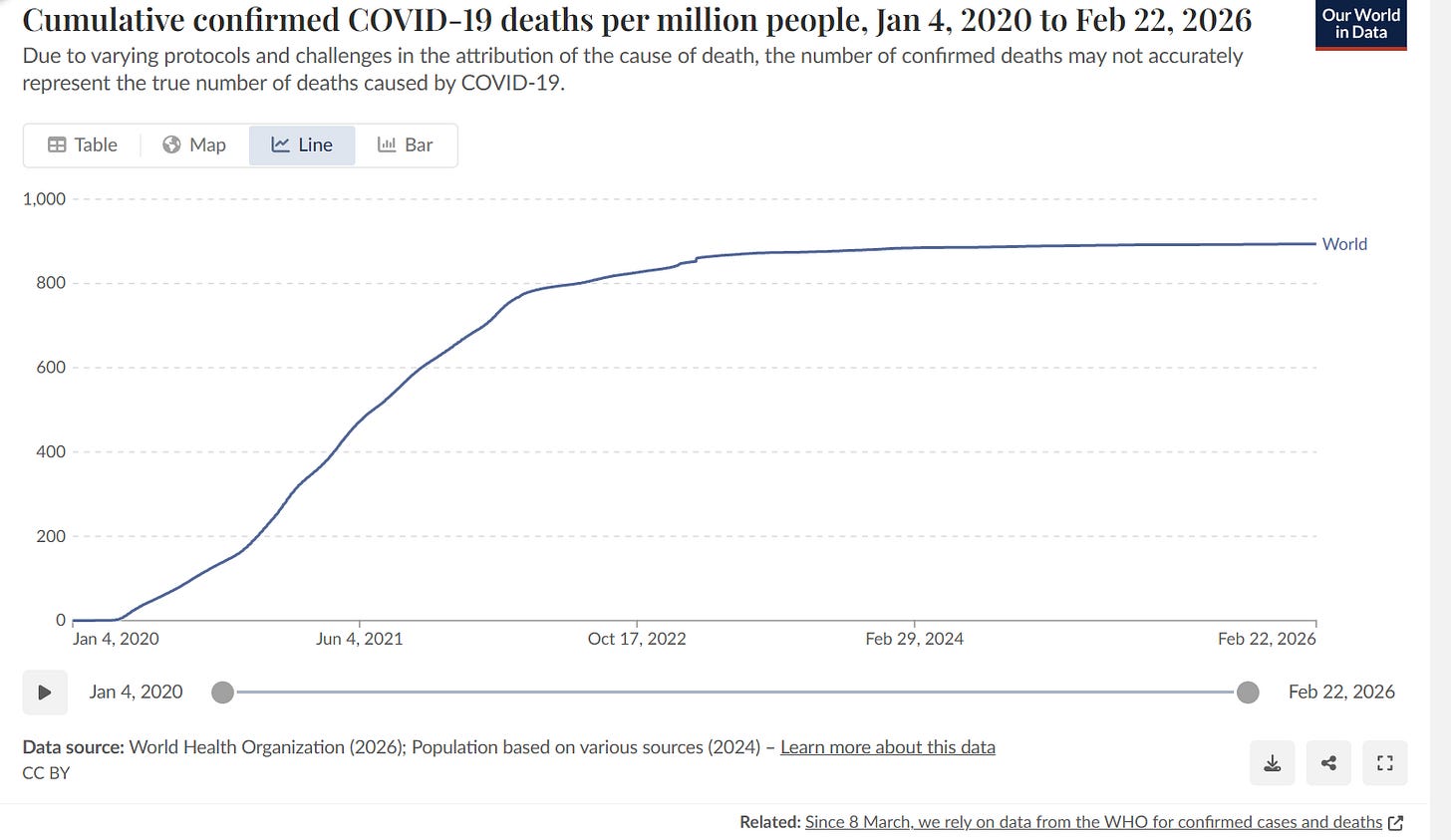
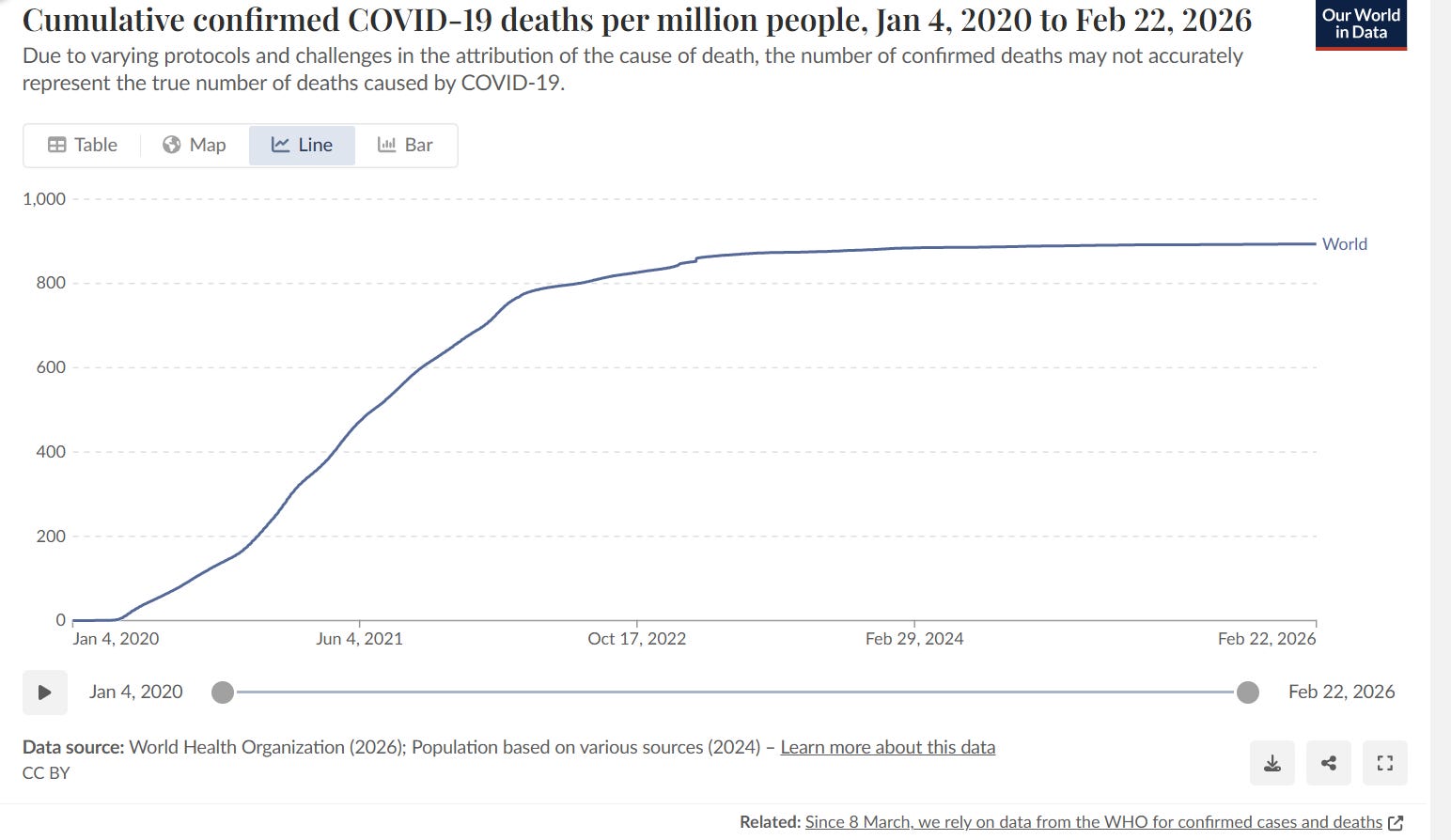
No effect worldwide of the vaccine: No “knee” in the cumulative COVID death curve as the vaccine rolled out worldwide.
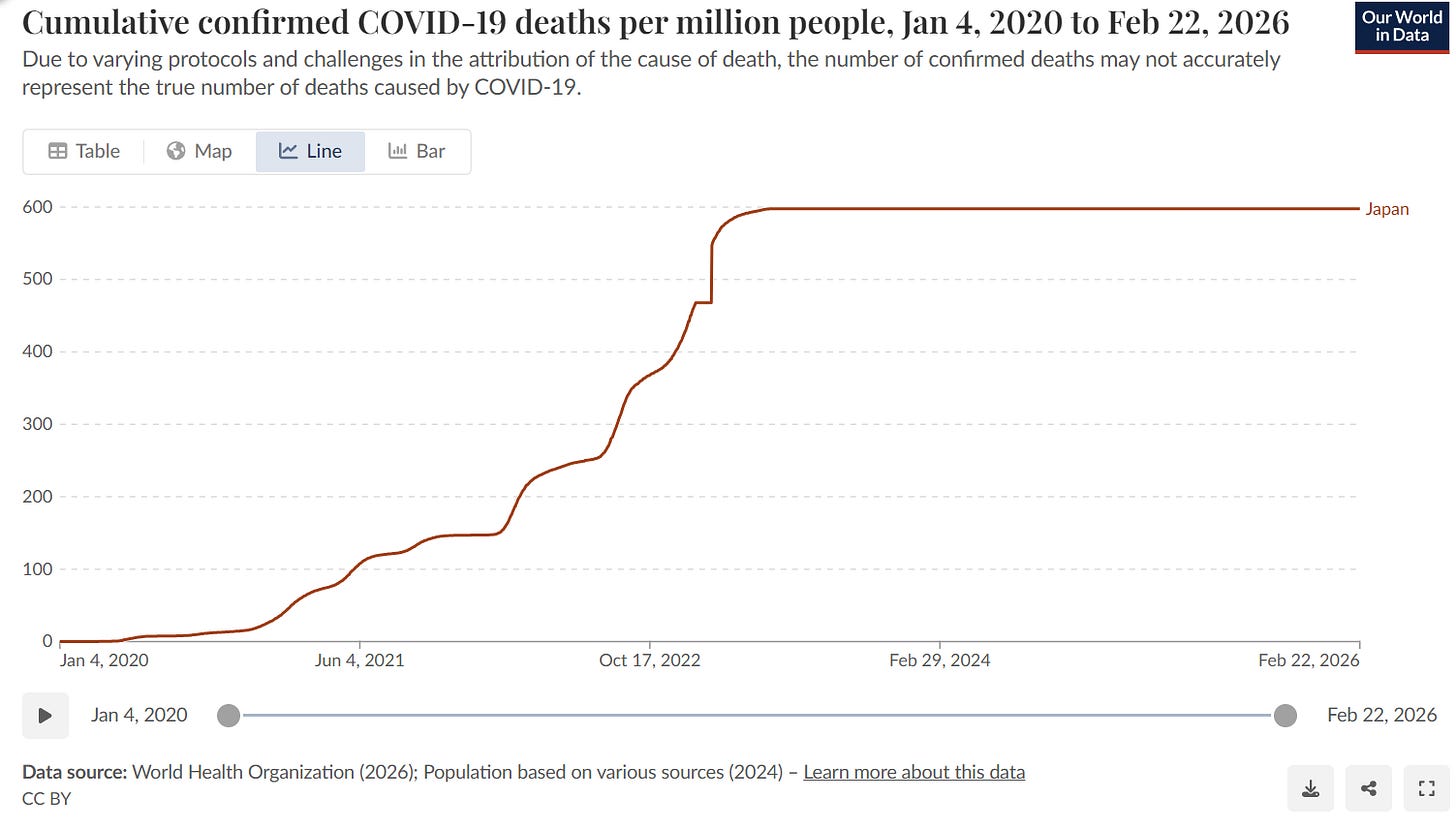
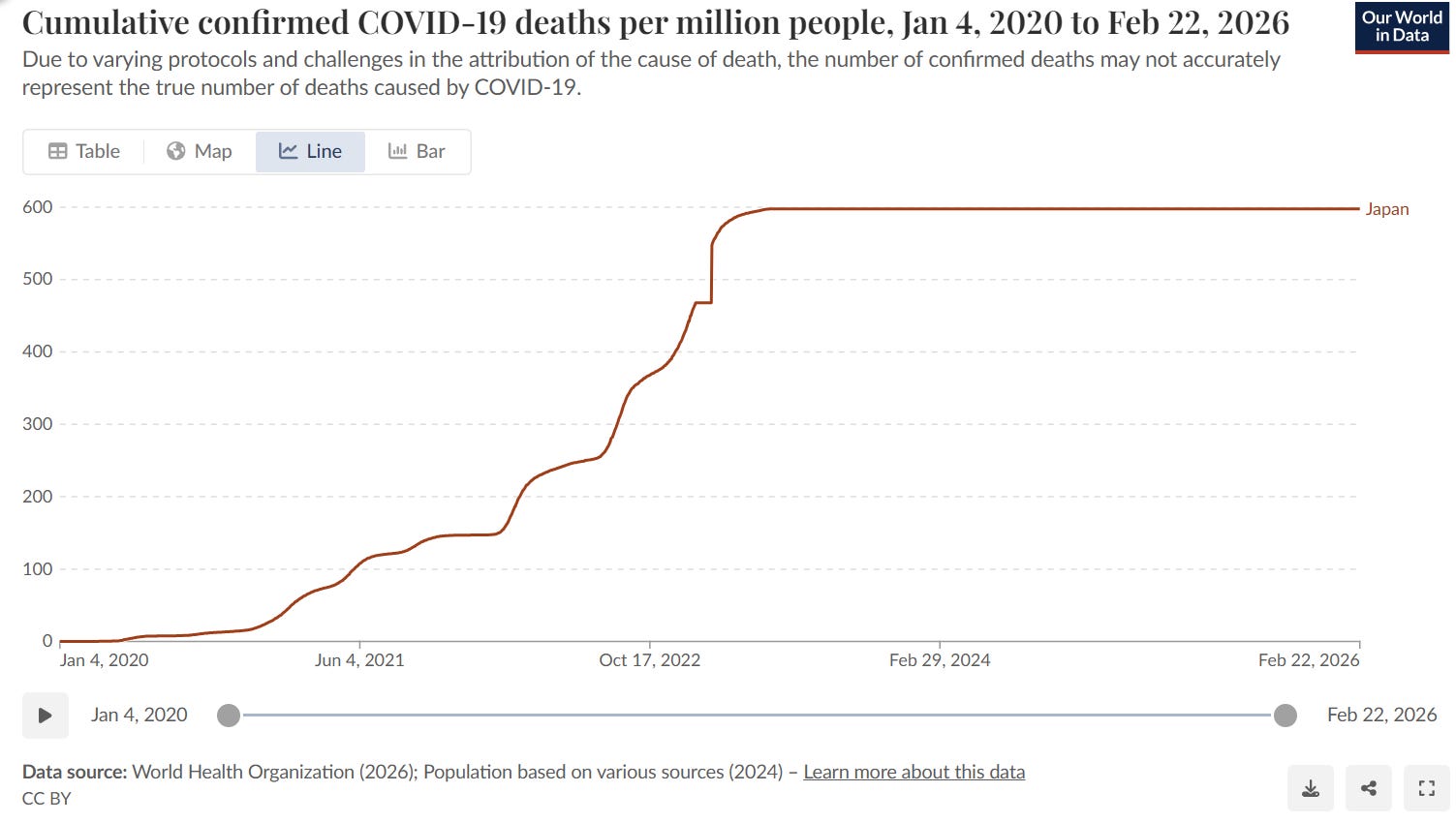
And in highly vaccinated Japan, instead of COVID cumulative death curves “flatlining”, they did the opposite and got steeper over time! Whoops! How can THAT happen?!?
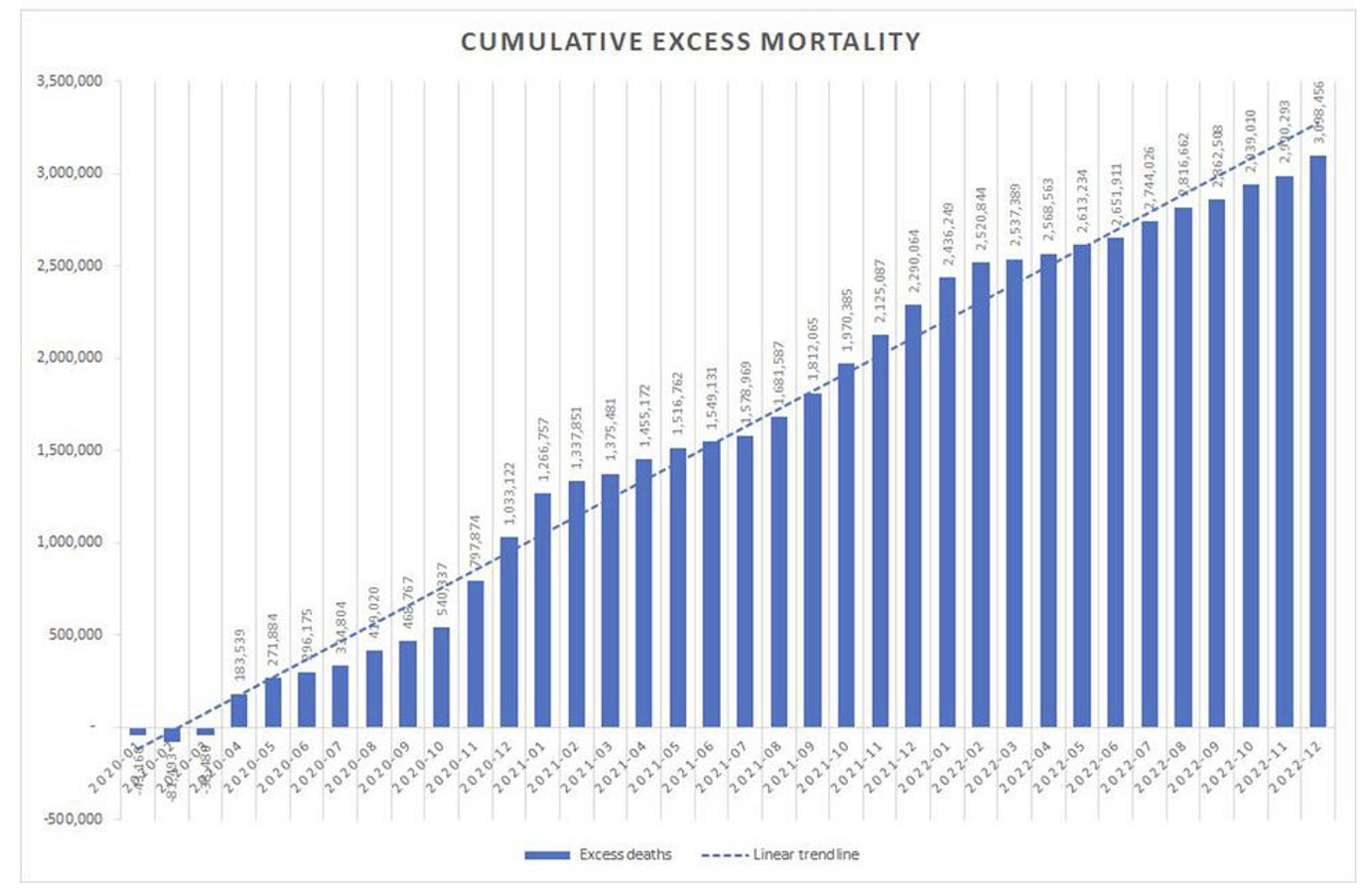
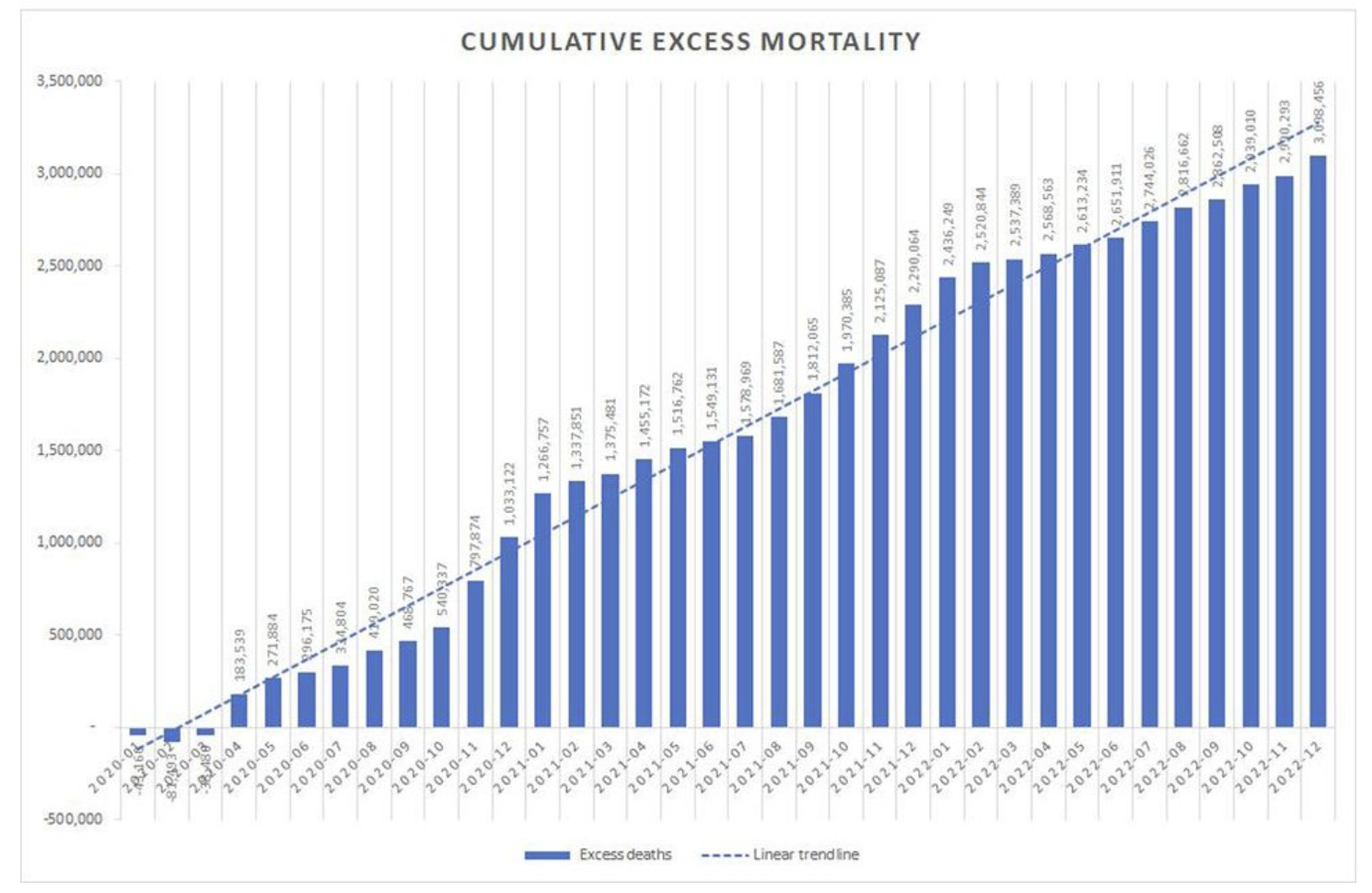
And the Mostert study showed excess deaths kept rising worldwide instead of turning around
And now the Czech data shows no benefit as well!
Czech Republic record level data
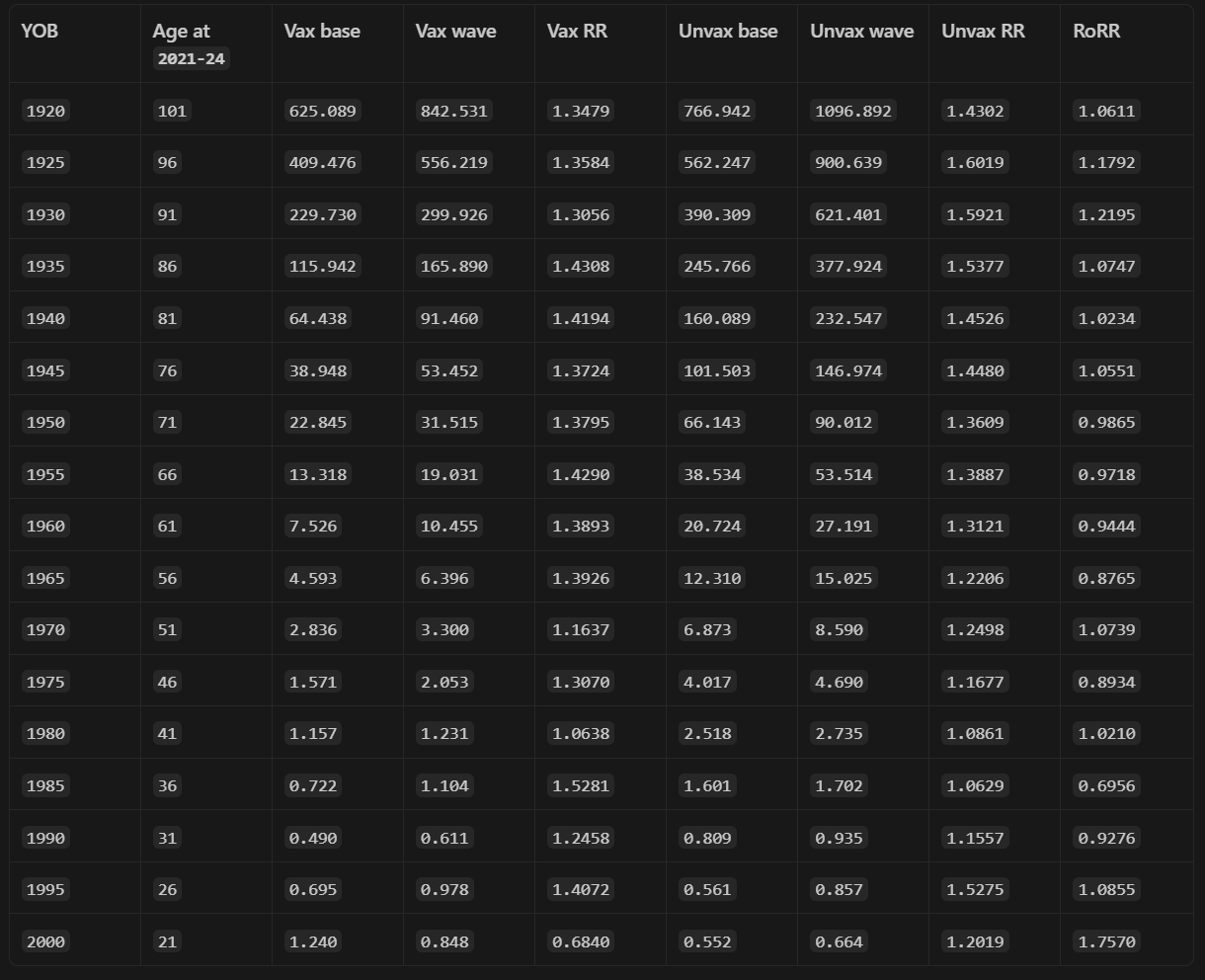
This table reports the Czech
2021-24fixed-cohort all-cause mortality check used above. Rates are all-cause deaths per100,000person-weeks. The baseline window is ISO weeks2021-24to2021-40; the wave window is2021-41to2022-17.RoRRis(wave / baseline in unvaccinated) / (wave / baseline in vaccinated). ARoRRabove1.0means the unvaccinated cohort had the larger wave-to-baseline mortality increase; here, the headline intervals include1.0, so this is not a precise causal effect estimate. This is a Czech record-level stress check, not a U.S. national causal estimator. RoRR=ratio of rate ratios and is the standard epidemiologic measure.
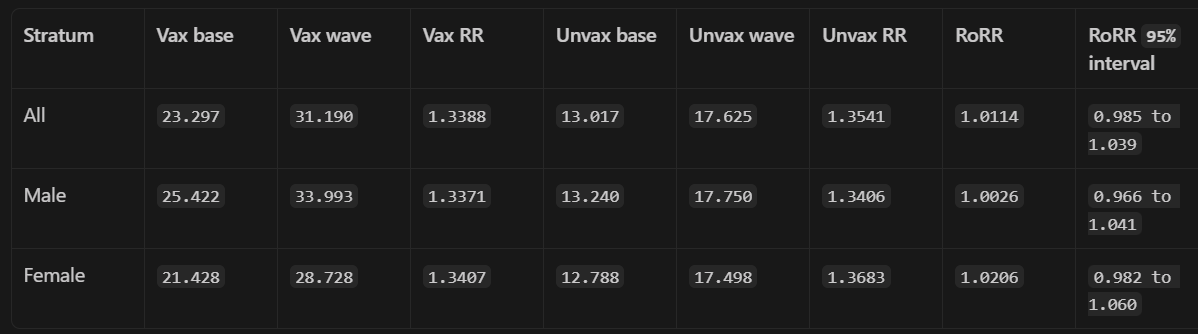
The all-sex birth-year rows below show why the headline result is not simply an aggregate-composition artifact. Unvaccinated baseline mortality is often much higher than vaccinated baseline mortality within the same birth-year band, but the wave-versus-baseline rate-ratio contrast remains mixed rather than showing a stable vaccinated advantage. Birth-year intervals are omitted below for readability; sparse younger cells should be treated as descriptive and high-variance.
Baseline choice
Suppose you do a sensitivity check by looking at the results with different baseline choices where you enroll and take the baseline on enrollment date. Red means the vaccine was protective, blue means the unvaccinated did better.
This is why you want to choose the whole non-COVID period as the baseline rather than cherry pick a specific date.
But the larger point is this: if the vaccine was really as effective as has been claimed, cherry picking a baseline should make no difference in the sign.

Taking a baseline after the COVID wave
The last loop hole is the claim of selection effects. If you take the baseline AFTER the COVID wave, the unvaccinated group can appear to have up to a 30% higher rise in ACM than the vaccinated group. But there is a 2x difference in mortality rate for people of the same age and the Levin paper implies a 1.49 non-proportional hazard effect size and 2**.49 is basically sqrt(2)=1.4 so we’d expect to see a 40% higher higher rise in ACM so a value of 1.3 is actually well within bounds of “no benefit.”
Even the most vaccine-favorable Czech post-wave contrast produces only a 1.325x unvaccinated/vaccinated wave/post all-cause mortality multiplier. That is smaller than the conservative Levin-style NPH/frailty correction implied by a 2x baseline mortality imbalance (~1.4x), and far smaller than the full COVID-risk scaling implied by the Levin age slope. Therefore the post-wave contrast does not rescue a clean vaccine-benefit interpretation; it remains well within the range that baseline mortality imbalance and non-proportional COVID risk could generate.
Here’s the detail:
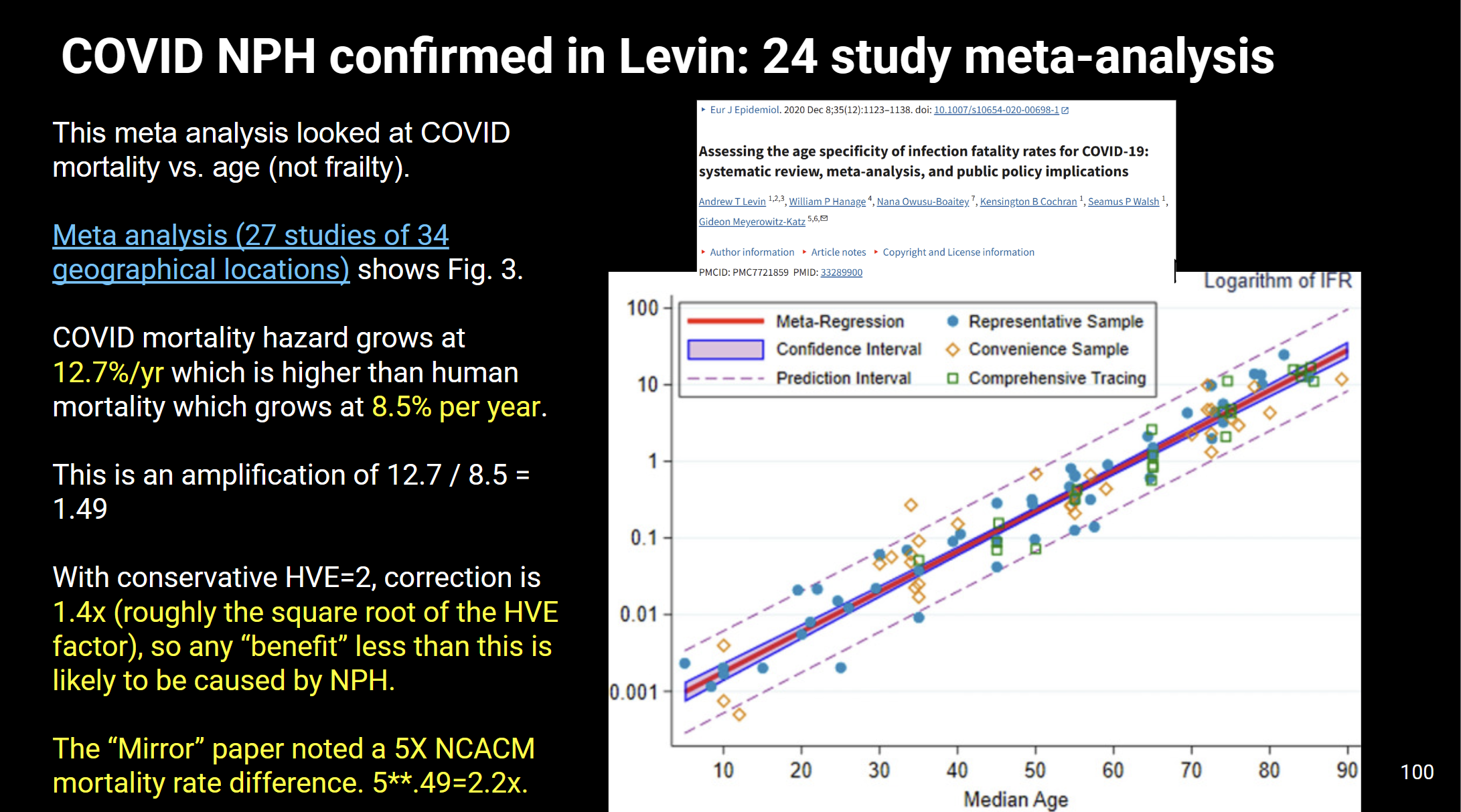
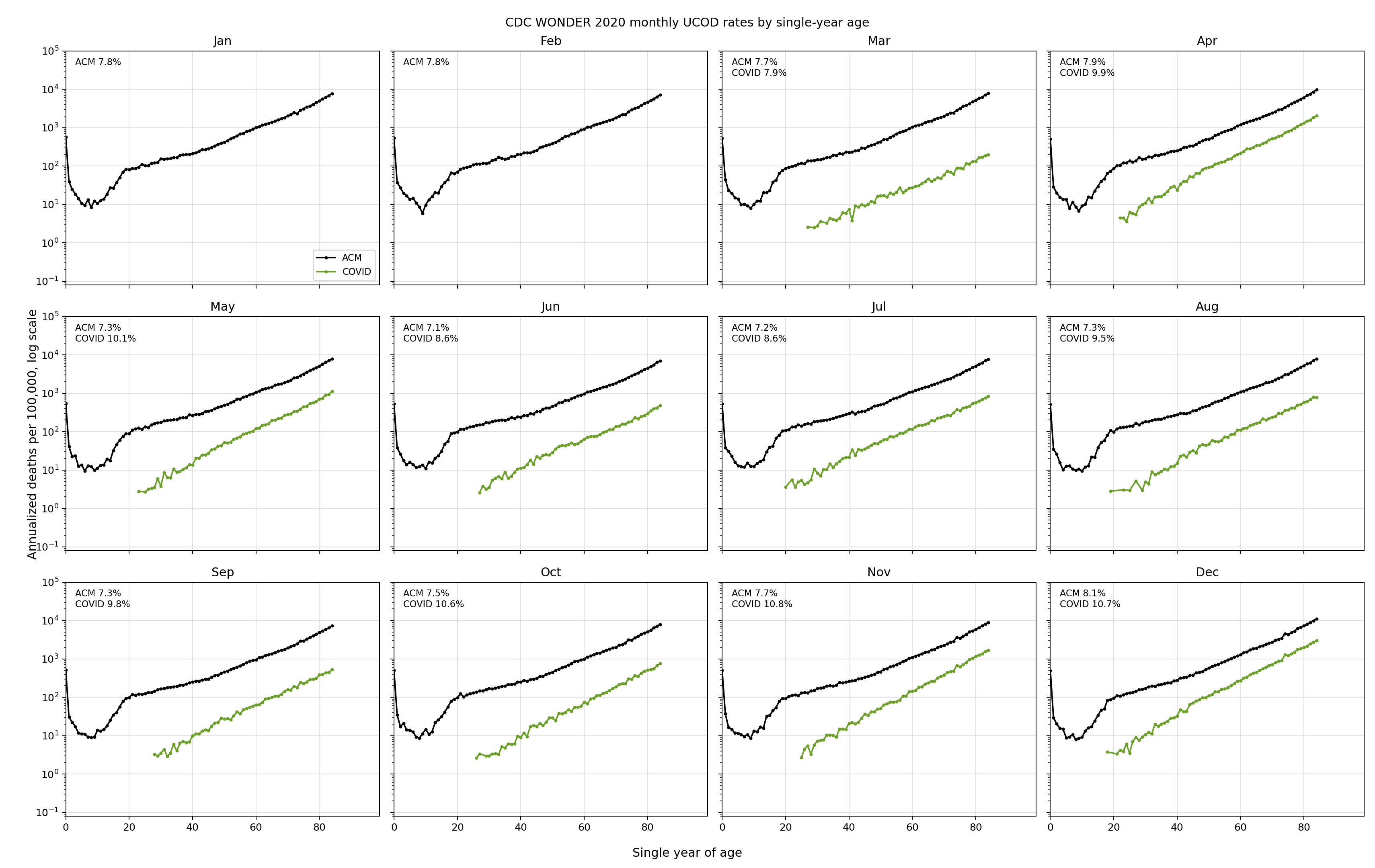
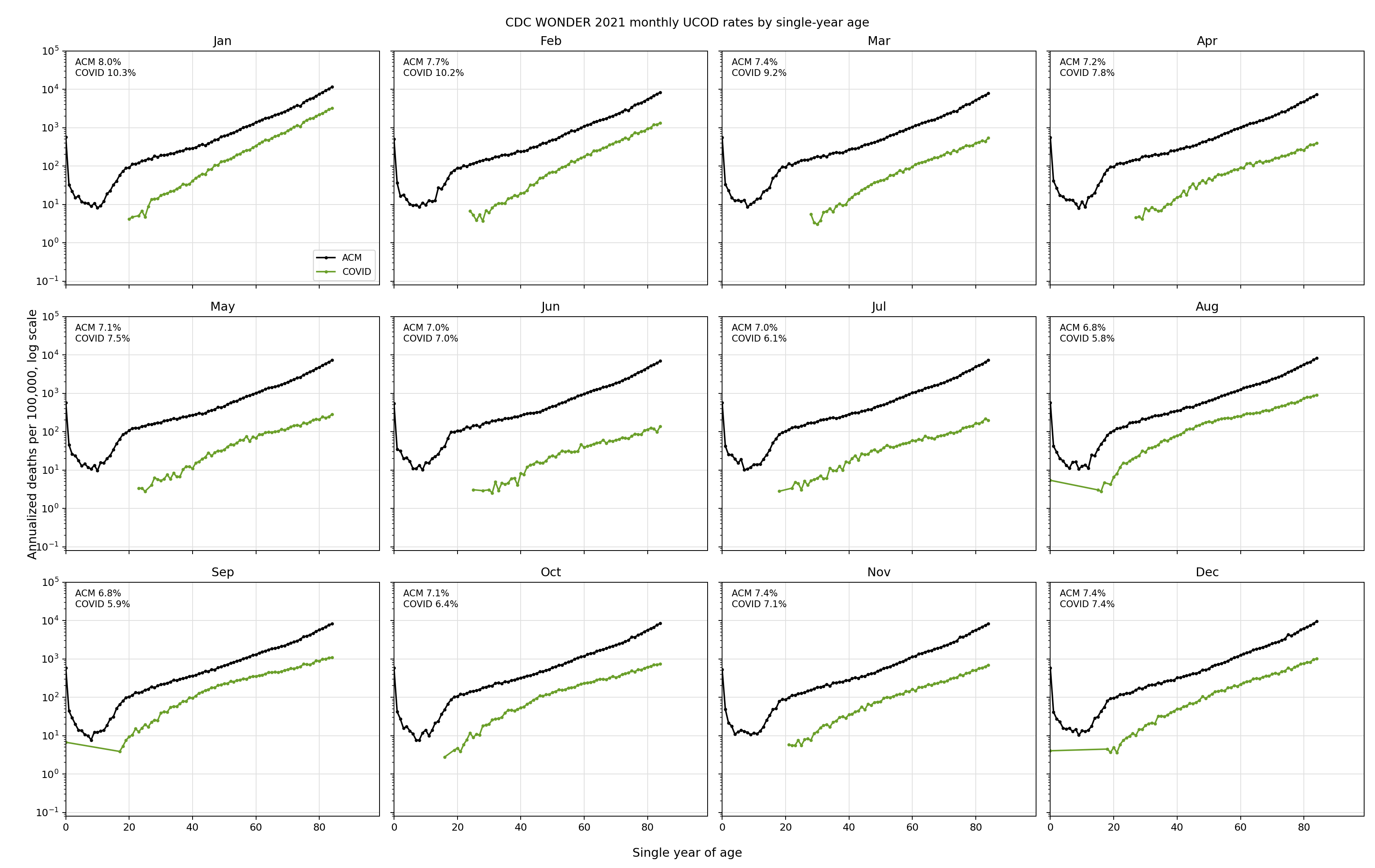
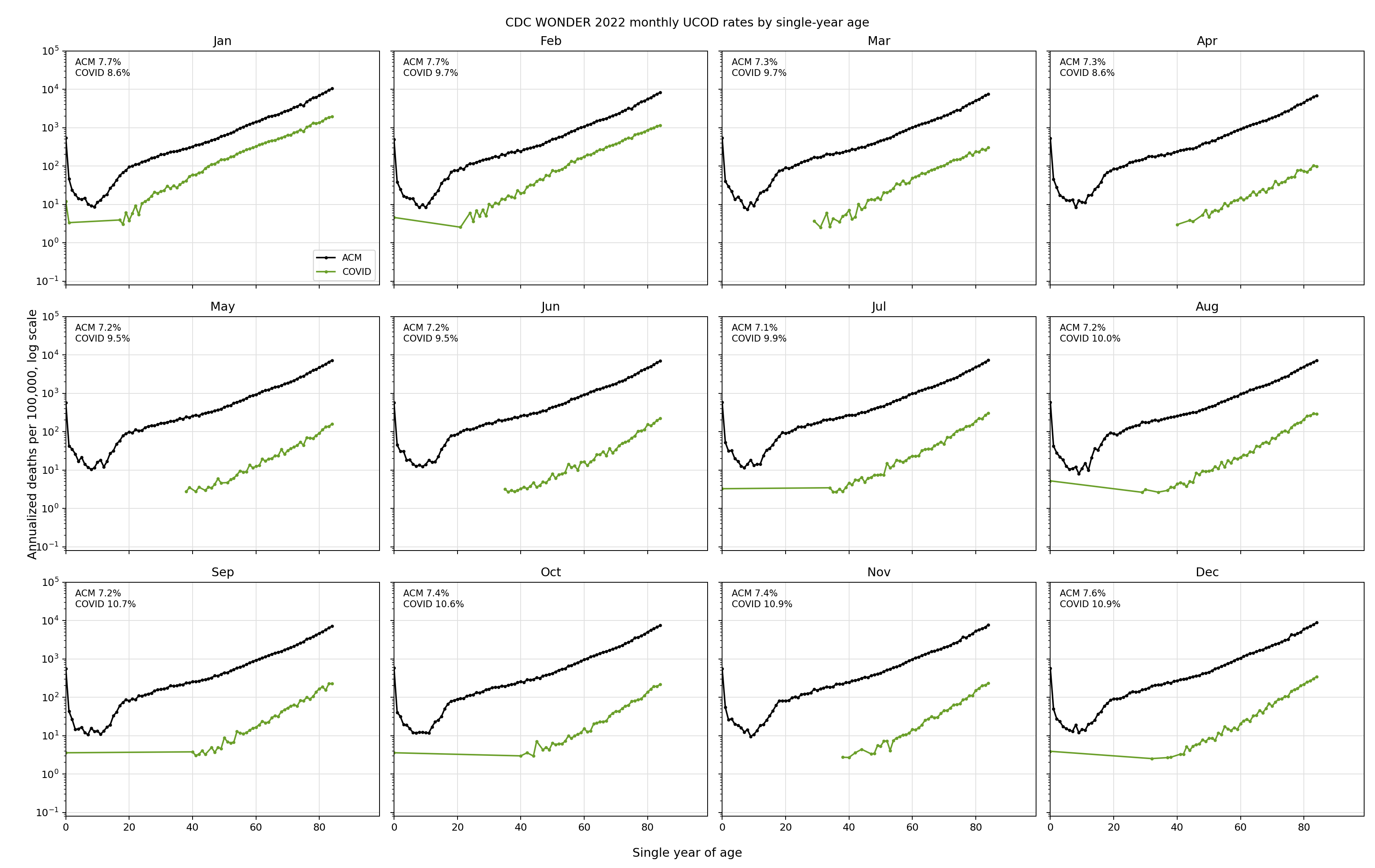
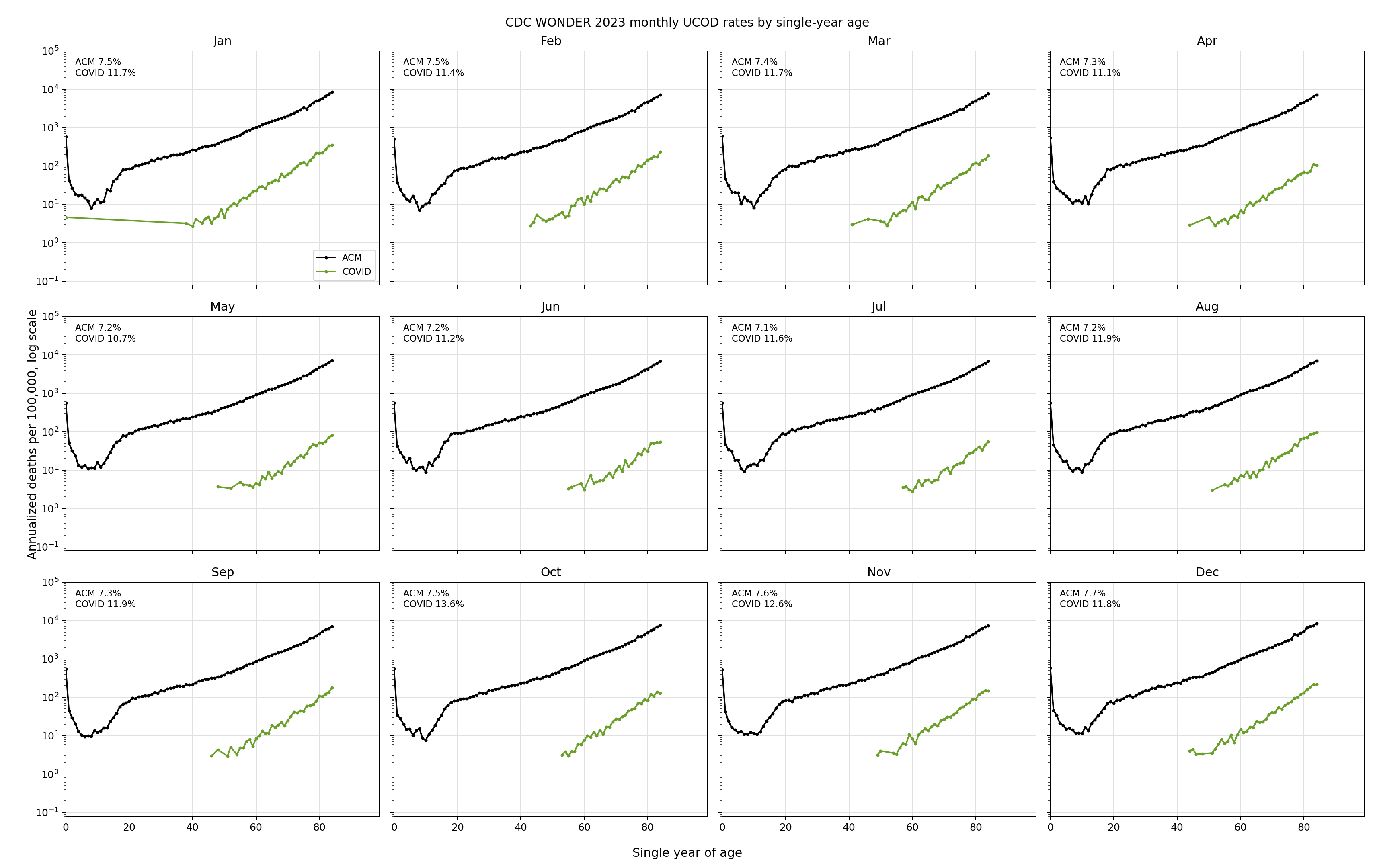
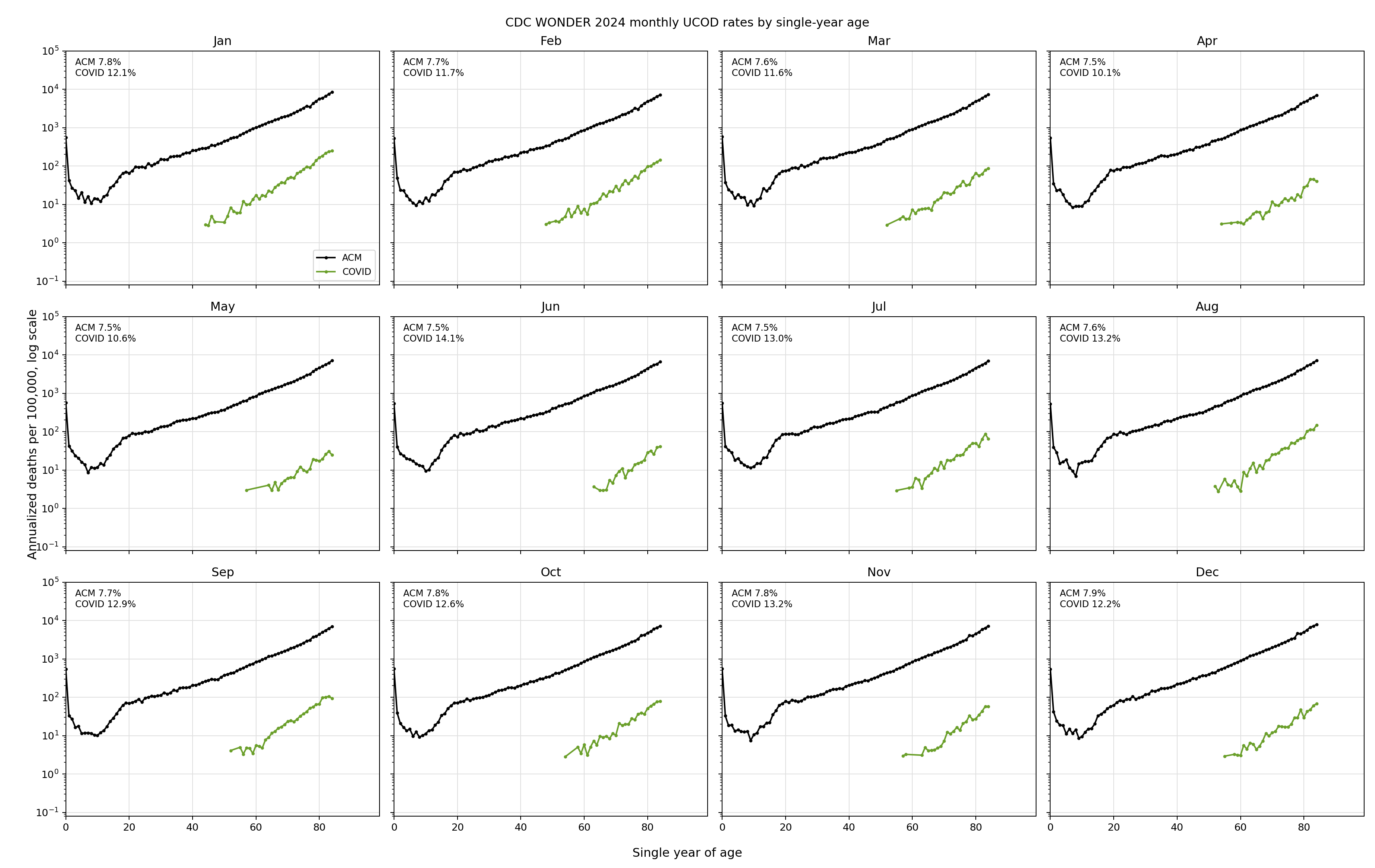
Using CDC UCOD data to validate NPH values in Levin
Using the US data in UCOD, we can plot the COVID vs all-cause mortality (including COVID) for various years to see that in all but 5 months, COVID had a steeper slope than ACM. The maximum slope difference between the COVID slope and all cause mortality slope was 14%/yr vs. 7.5%/yr.
Attacks by critics
Henjin and Timberlake using analysis from Henjin) claim the Czech data shows the vaccine worked.
Yet they don’t identify an error in my methods or computations since I do the baseline computation before and after the COVID wave making it completely fair.
Both of them ignore the NPH effect completely.
From ChatGPT:
Their critique does not identify an arithmetic or cohort-construction error. It substitutes dynamic vaccine-status/product plots for a fixed-cohort all-cause mortality estimand. Those plots may be useful descriptively, but they are not cleaner evidence of vaccine benefit because they remain exposed to time-varying selection, product-channel allocation, recent-dose HVE, and baseline frailty differences. When the claims are tested under a fixed 2021-24 cohort with person-week denominators and washout checks, they do not recover a stable all-cause mortality benefit.
They appear to be arguing:
There is a visible vaccinated/unvaccinated or product-group difference during the COVID wave.
That difference should be interpreted as vaccine benefit against COVID mortality.
Your ACM comparison is misleading because HVE/product timing/post-wave baselines complicate it.
But the data they are pointing to are not fixed-cohort causal estimates. They are dynamic vaccinated/unvaccinated or first-product curves, which are exposed to:
changing membership over time;
recent-dose healthy-vaccinee effects;
product allocation/channel effects;
age/frailty differences within age bands;
survival/depletion effects;
later doses and product switching;
calendar-time differences;
COVID infection history differences.
Summary
The Czech Republic record level data is a stunning confirmation of “no COVID mortality benefit” for the COVID shots. All you had to do is ignore the “label” of a COVID death and simply look at all-cause mortality during non-COVID period vs. COVID periods for the vaccinated vs. unvaccinated.
I’m not aware of any other publicly available record level dataset that can be used for this test although the US Nursing home data is quite good if we use it longitudinally to monitor the case fatality rate (CFR) during the rollout.
So the Czech data remains the best (and only) public dataset for computing the COVID mortality benefit. I’m not aware of any dataset that would be more dispositive showing a different result.
So no significant COVID benefit.
On the harm side, we have the Levi/Ladapo Florida study and confirmation of similar death numbers from the Skidmore paper, VAERS, Rasmussen public surveys, and more.
If the COVID vaccine was so beneficial, why do the authorities need to keep the data hidden from view? Baffling isn’t it???
The bottom line is this: the best quality datasets for answering questions of benefit vs. harm all say the same thing for the COVID vaccines: harms >> benefits.
Its really amazing how the only country to release actual data is the Czech Republic. It says a lot about just how corrupt the whole global system is.
The non-release of Covid data reminds me of how the CDC has delayed the release of cancer death data. Utter incompetence - or - "something" is causing a cancer pandemic and the CDC doesn't want us to know. Tuskeegee is now happening to everyone, because nobody was punished the last time it happened.
https://www.cdc.gov/cancer/data/index.html
2022 is the latest year for which cancer incidence data are available; 2023 is the latest year for which cancer death data are available.
Hi Steve,
I appreciate you continuing to speak truth, and show the real science.
I first learned about you and Substack because of the movie, "Died Suddenly". I can't seem to find that movie anywhere. Is it possible for you to show that movie on your Substack? I think it would be good for people to see it again or for the first time.