
Initial analysis of record-level data from Czech Republic FOIA proves that the Moderna vaccines increased all-cause mortality by over 30% (and the Pfizer vaccines weren't safe either)
"Safe and effective?" Using this new data, we can finally prove that the COVID vaccines were not safe or effective for anyone of any age. No COVID benefits, and they increased your risk of death.


About the Czech Republic data article series
This is the original article that was first published on July 17, 2024.
The comprehensive summary is here: A summary of why the Czech Republic data is so devastating to the "safe and effective" narrative.
Scientific paper being drafted
Karl Jablonowski, Ph.D and Brian Hooker, PhD are in the process of writing this up for publication in a peer-reviewed journal.
About this article
Record-level vaccination-death data obtained legally under FOIA from the Czech Republic can be easily analyzed to compare the one-year mortality rates for each individual age group by brand. If the vaccines are all safe, the mortality should be very similar, differing only by marginal effectiveness. If we exclude months of COVID mortality, the mortality rates between brands should be nearly identical, only differing due to very small composition differences between participants in each age group of the same sex and age.
Unfortunately, the brands differ substantially whether or not you exclude the COVID months of death.
The importance of this article is that it proves, for the first time, using gold-standard unimpeachable data and a new brain-dead simple analysis method that is not subject to confounding, that the COVID vaccines increased all-cause mortality.
This article will be ignored by the mainstream media and medical community for as long as possible. This is why it is important to spread the word.
Executive summary
Official government record-level data obtained through a FOIA request from the Czech Republic shows that the Moderna COVID vaccine increased all-cause-mortality (ACM) as measured over a 12-month period from the time of vaccination for every age as compared to the Pfizer vaccine.
If the COVID vaccines were safe, the overall ACM across different vaccine brands would be very similar.
This is not the case. They are radically different and the difference is highly statistically significant.
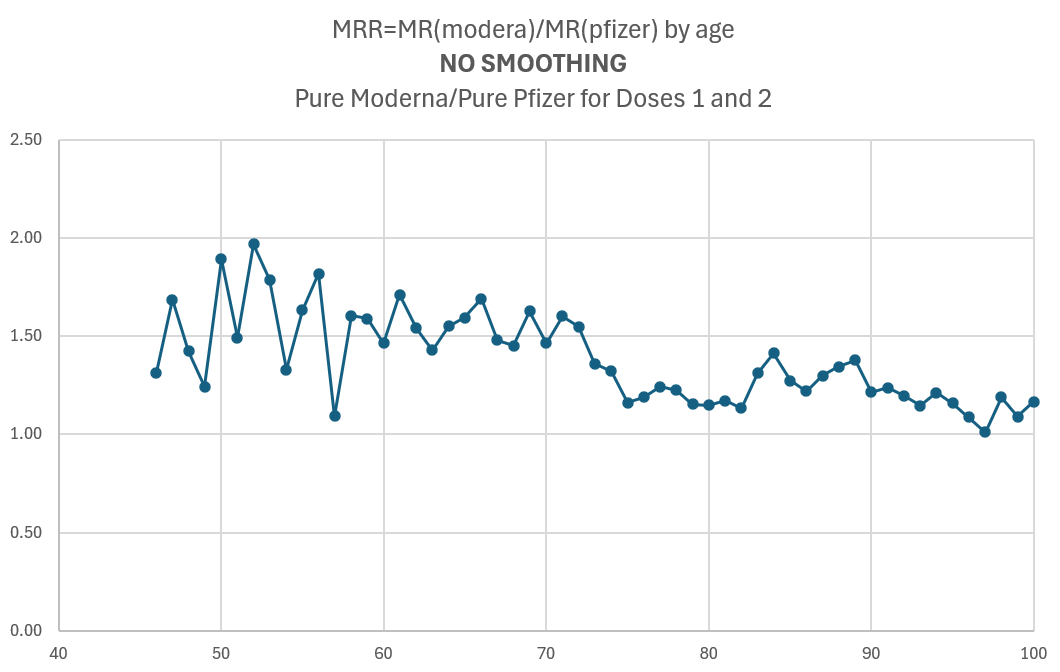
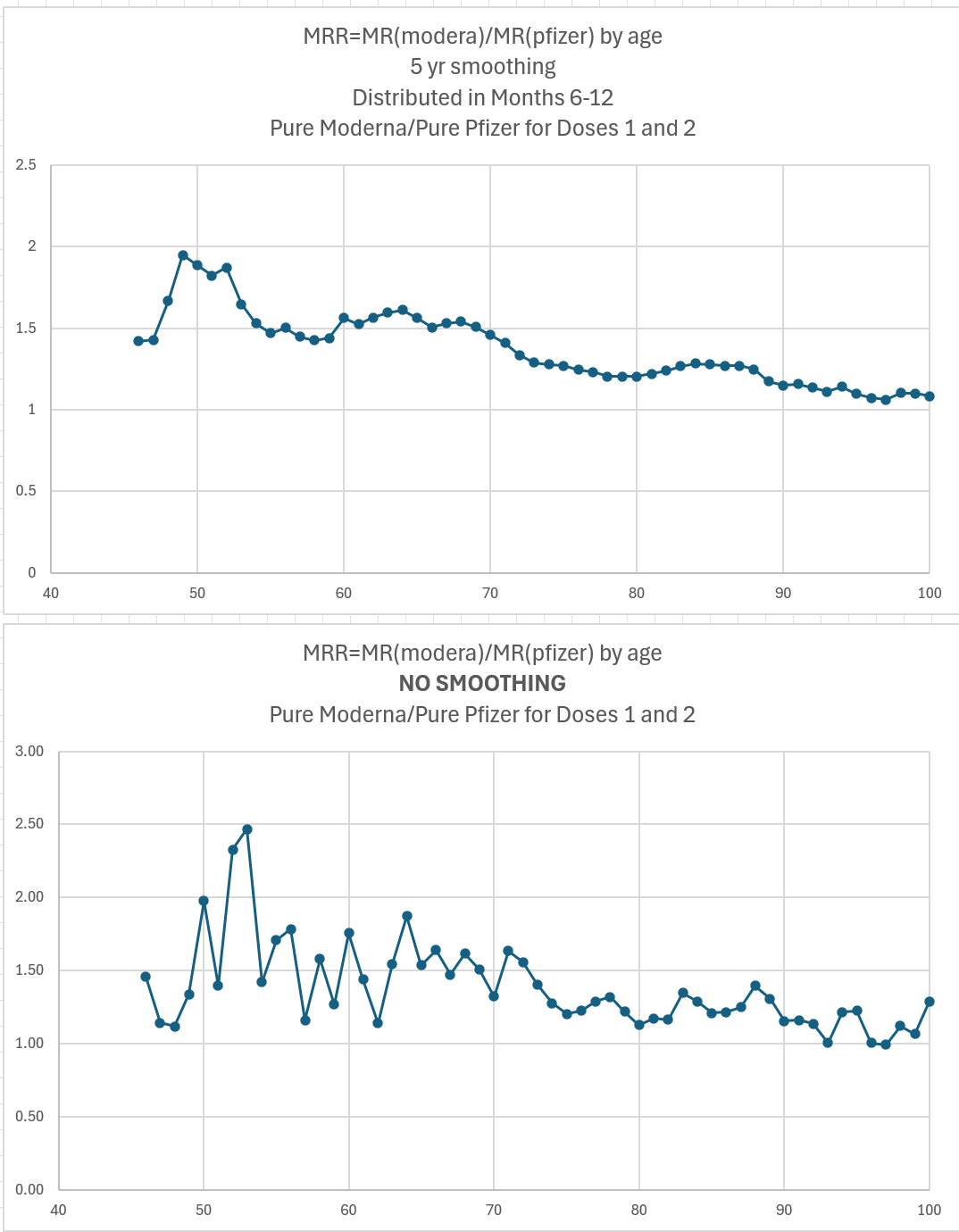
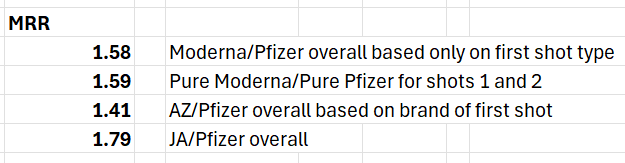
For example, for ages 46-69 who got two shots of Moderna vs. two shots of Pfizer in 2021 in the Czech Republic, there is over a 50% higher risk of death measured over a 1 year time window since the time of the shot as shown in the chart above.
The younger you were, the greater the percentage increase in risk. For 20 to 29 year old’s for example, the MRR (mortality rate ratio between Moderna to Pfizer) approached 2:1 which means you more than doubled your all-cause mortality if you took a Moderna shot.
So even if the Pfizer vaccine was 100% safe, the Moderna vaccine should be immediately stopped as being far too deadly to use for any age group.
The 50% number is an absolute ACM increase compared to the Pfizer ACM value, not a comparison of excess mortality risk.
That’s a train wreck. Vaccines are always supposed to reduce absolute ACM. Vaccines are never supposed to increase ACM, even by a little bit.
The Pfizer COVID vaccine is also too unsafe to use, but we don’t have enough data to accurately estimate how much it increases all-cause mortality. From the limited data, I believe it’s safe to say Pfizer appears to have at least 10% higher all-cause mortality than Novavax (that is a very conservative estimate since all the data was much higher than that), making Pfizer also completely unsuitable for public use.
To put it in numbers, if everyone in the US got the initial 2 dose Moderna shot, it would cause a minimum of 650,000 excess deaths (which I estimated at a 20% increase in overall US ACM because the ACM rates are much higher for older ages where the % impact of the vaccine is much smaller). That is a conservative estimate. Rancourt et al estimated the COVID shots kill on average for all ages 1.26 people per 1,000 shots. In the US with over 677M shots given, the estimate is over 850,000 deaths.
Even more problematic is that no world health authority, local, national, or international, was able to detect such a massive relative mortality increase of Moderna compared to Pfizer.
The reason is simple: none of them bothered to look.
There isn’t a single mortality comparison by brand posted by a public health agency anywhere in the world ever. Not even in internal documents.
That’s appalling. Yet nobody in the mainstream medical community ever voiced a concern about the lack of this sort of obvious safety monitoring and the total lack of data transparency.
If they looked, they would have found exactly what I found: a major problem. It took me less than 15 hours from the time I got the data to spot the huge anomaly in the data.
This is a major failing of the medical community and regulators. They should all publicly apologize and admit they were inept.
If Moderna cannot show how this analysis is wrong, then the Moderna vaccines should be immediately halted worldwide to prevent further deaths.
All the source data and analysis tools are in full public view for anyone to replicate.
I’ve reached out to Pfizer, Moderna, Novavax, and UPenn Biostatistics Professor Jeffrey Morris for comments on this article.
Only Professor Morris replied. I’ve included a link to his analysis of this article so you can decide for yourself. He basically has no issues with the data integrity, the methodology, or the results of applying the methodology to the data. He believes my interpretation of the results are flawed; the vaccines are safe and that there must be a confounder that explains why there is a disparity.
Here is everything you need to know: Professor Morris cannot explain why, if the COVID vaccines are safe, there can be a 50% higher mortality rate if you got a Moderna shot instead of a Pfizer shot. And for why younger people had even greater mortality disparities. Even in his explanation posted on X, he tries to distract your attention, and completely avoids trying to explain the key point of this article. He now admits I am right, that Moderna has higher death rates than Pfizer, but then says that the death rates are still lower than the unvaccinated so that the COVID vaccines saved lives and that Moderna saved fewer lives than Pfizer.
But the problem of course with his logic is that there is no evidence whatsoever that the mortality differences between the brands were during the COVID waves where, if he’s right, Pfizer deaths didn’t go up and Moderna did go up. The time series below show the mortality differences emerged as soon as you got the shot and for each of the next 20 weeks after that. And Dr. Clare Craig addressed the COVID differences in her post (there were none).
And this is precisely why this article is so important: Because there is no viable explanation for the Czech Republic data other than the obvious explanation: that the Moderna vaccine is far more deadly than the Pfizer vaccine.
Note: This is a living document. I will be updating this article with new data and if there are any mistakes I will fix them.
The video
There is a one-hour video of me explaining the data, the methods, the results, and the implications on Rumble.
Here’s a 90-second video showing why you should never trust the medical community ever again when they say something is “safe and effective.”
Outline
This may be helpful in navigating this document. Key sections are:
Data source and characteristics
Methodology
Results
Interpretation
Third-party analyses
Implications
Attack vectors
Actions that should be taken in response to this data
Predicted reactions from FDA, CDC, Moderna, …
The stunning attempt to debunk this analysis from UPenn Director of the Division of Biostatistics Professor Jeffrey Morris
Testimonials
Acknowledgements
Next steps
Introduction
The Czech Republic official record-level data on vaccines administered to the entire country has been sitting on the Internet for nearly 4 months. I just found out about it.
This data is the mother lode. We have NEVER had data like this before.
Because there was no systematic bias in the way the vaccines were allocated in the Czech Republic, calculating the 1 year mortality rate (MR) of each age group from the date of the shot should yield very similar numbers for each vaccine brand if the vaccines are safe. The MR=(# died within 1 year)/(# injected).
Let’s define a mortality rate ratio or MRR = MR (Moderna) / MR (Pfizer).
If both vaccines are safe and reduced all-cause mortality by similar amounts, the MRR will be approximately 1 for all age groups.
But what we found is stunning. The numbers are not similar at all.
Moderna has over a 50% higher all-cause mortality for ages 46-69 than Pfizer.
Even if Pfizer reduced all-cause mortality by 10% for all age groups (which is completely improbable as I’ll show in a subsequent article), Moderna would still have increased all-cause mortality and should be immediately pulled from the market worldwide unless Moderna can explain how the Czech the data is consistent with a safe vaccine.
I don’t see how they can possibly do that.
Furthermore, this data should completely decimate any trust anyone had in the medical community to monitor vaccine safety and protect the public. If after 3.5 years of data collection you cannot detect a vaccine which increases all-cause mortality by 50% or more, you should admit you are completely incompetent to monitor for vaccine safety.
In addition, the medical journals should retract all studies showing the COVID vaccines are safe. They are not. All of these studies are false and misleading.
Pfizer is unsafe too (it increases all-cause mortality by 10% or more), but I’ll cover that in a subsequent article.
Getting the data
I’ve posted the Czech Republic data and all the analysis tools I used to my github repo. Anyone can download and verify the results in under 1 hour. The analysis directory has various spreadsheets allowing you to verify, analyze, and visualize the data.
The data was originally obtained by a Czech citizen (Stanislav Veselý) under a FOIA request. Tomáš Furst posted it to github 4 months ago on March 29, 2024 but he didn’t tell anyone and nobody noticed.
About the data
This is official government data on everyone in the country.
The data includes everyone who was alive at any time during the period from 2020 onwards. This means that it has more rows than the number of people alive at any particular time point. Those who died during that period and those who were born during that period are included. The data matches the numbers reported by the Czech Bureau of Statistics.
Exact dates are provided for everything except date of birth. To preserve privacy, they just supplied the year of birth.
The data has one record per person showing up to 7 vaccinations
Each vaccination record consisted of 4 fields: date of vaccination, lot number, vaccine code, and vaccine manufacturer.
If the person died between Jan 1, 2020 and December 31, 2022, the exact date of death was supplied. People who died before this period are not included in the data. People who died after are included but their death is not recorded.
This is gold-standard data. Official data. Over 5M vaccinated. We have never had a publicly available database before with record-level data like this allowing us to accurately compare mortality between vaccine brands.
Methodology
In this retrospective study, I defined 3 study groups:
Study 1: Got shot #1 in 2021 of a COVID vaccine
Study 2: Got shot #2 in 2021 of a COVID vaccine
Study 3: Got shot #3 in 2021 of a COVID vaccine
When people met the criteria they were enrolled in the study. We then tallied for each date of birth, the number enrolled and the number who died within 1 year of enrollment.
The mortality rate (MR) of a vaccine for those born within a given calendar year was defined as the number of people who died within a year of the shot divided by the number of people enrolled.
The MRR is defined as the MR (Moderna)/ MR (Pfizer). This is an absolute mortality ratio, not an excess mortality ratio.
If both vaccines are relatively safe, the MRR values should be close to 1 for every age.
In this article, I focus on comparing Pfizer with Moderna, but the underlying data was tallied for all vaccines.
Results
They are summarized in this graph which was calculated from those who were enrolled in Study 2 (i.e., who got two shots in 2021). To provide the best differentiation between the brands, the curve below was computed for those getting two shots of the same brand. In practice, very few people switched brands between the first shot and the second shot.
The MRR going down means the mortality impact was greater for younger people than older people. It was minimal for those aged 95 or older.
The details are in the spreadsheets in the analysis directory in my github.
The spreadsheet with these charts is called Analysis.xlsx. Go to the “MRR by YOB” tab to see these graphs above.
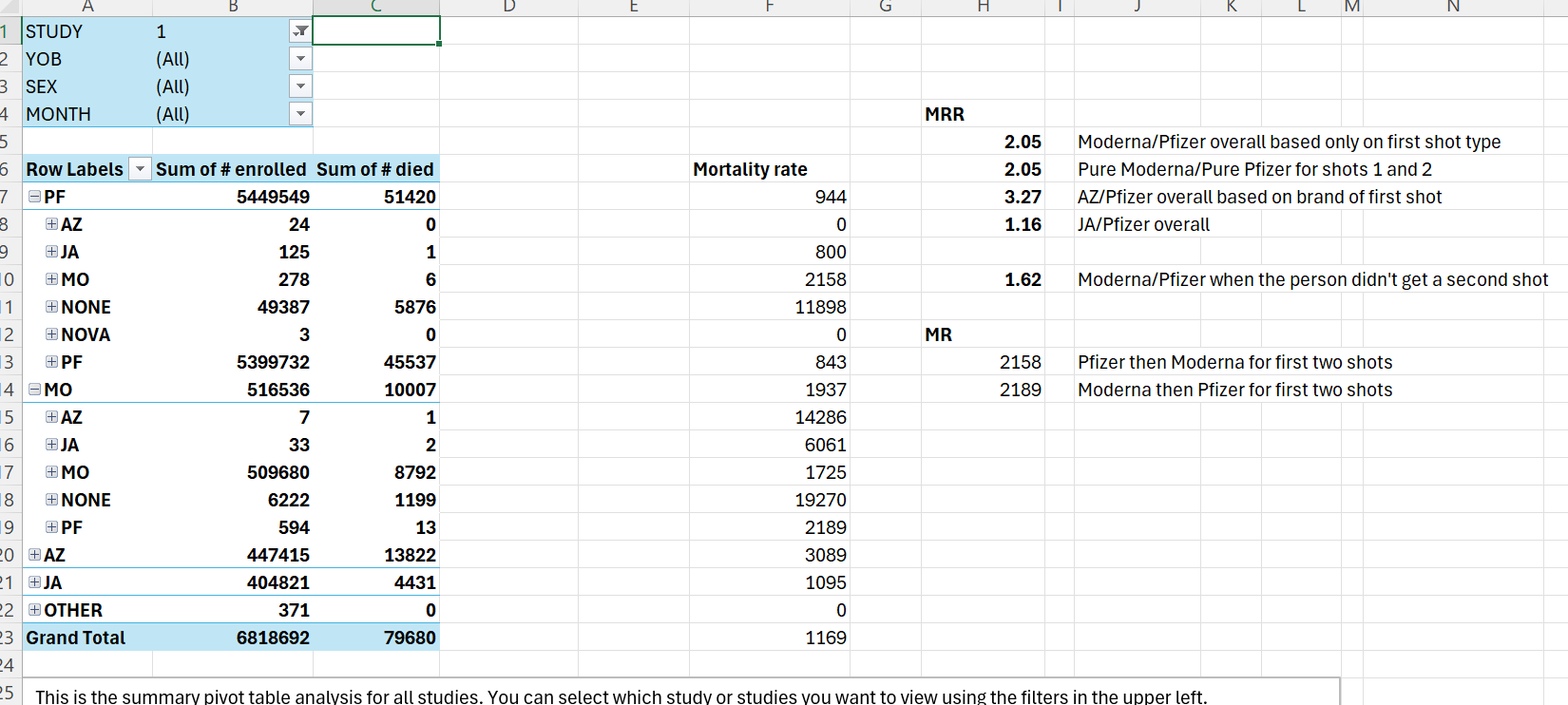
Check out the summary page as well where you can drill down and explore.
Dose 2 in June 2021 analysis
Could the numbers above be simply due to differences in vaccine efficacy during the COVID waves, e.g., Pfizer is extremely effective and Moderna not?
No, not really. You simply can get a 50% difference in mortality over a 1 year period even if Pfizer is 100% effective in preventing COVID deaths (which if true, everyone would notice and it lacks biological plausibility) and Moderna is 0% effective. You might be able to achieve 15% differences under the best cases, but people would have noticed the brand differences if nobody died from COVID who got Pfizer.
Also, there would be an extreme difference in the V-safe data for doctor visits between Pfizer and Moderna. Pfizer would have a tiny fraction of the safety reports.
And people who had friends who died from the shots would have 0 friends dying from Pfizer, and all their friends dying from Moderna.
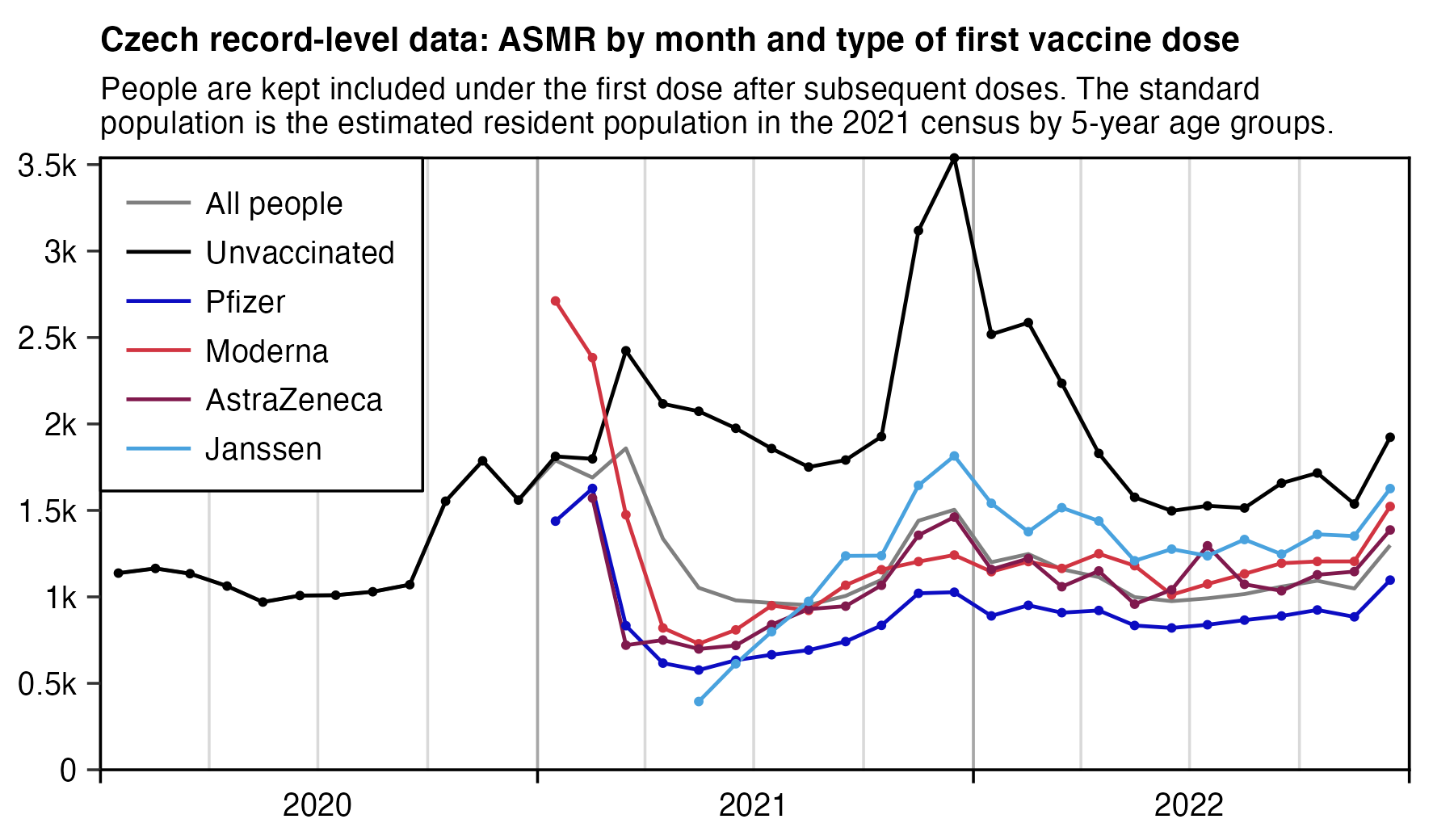
Henjin plotted an age standardized mortality rate plot (see section below) showing the unvaccinated vs. Moderna vs. Pfizer showing that the gaps don’t seem to change much over time. Can you determine high COVID (gaps should widen) vs. low COVID (gaps should disappear) from this graph by looking at the graph? You sure can’t! And that’s the problem, isn’t it? If the vaccines were safe and provided the same level of protection against mortality (which is what health officials claimed), then both vaccines should have lines that never separate hardly at all, and there should be a huge gap between the vaccinated and unvaccinated that widens during high COVID and narrows during low/no COVID. Clearly, this is not at all what happened which again proves that at least Moderna is not safe.
The high COVID periods can be seen from the OWID graph:

No COVID #1: June 1 to Oct 31, 2021
High COVID: Nov 1, 2021 - April 31, 2022.
Two COVID peaks: Dec 10, 2021 and Feb 18, 2022
No/low COVID #2: May 1, 2022 onward.
To resolve these questions, I created a Dose 2 given in Jun 2021 spreadsheet in the analysis directory of the github so we can compute the MRR during peak COVID and low COVID and we find that they are roughly the same meaning that there was no COVID mortality differential between the brands, it’s just noise.
The single most definitive observation about the data
As you can see from the “NO SMOOTHING” curve above, I computed the MRR in Study 2 for every single-year birth year.
There were 40 birth years where the Moderna deaths were >50.
Guess what? 40 out of 40 were >1!
If both vaccines are equally safe, the chance that Moderna would lose on 40 independent comparisons like this is about 1 in a trillion.
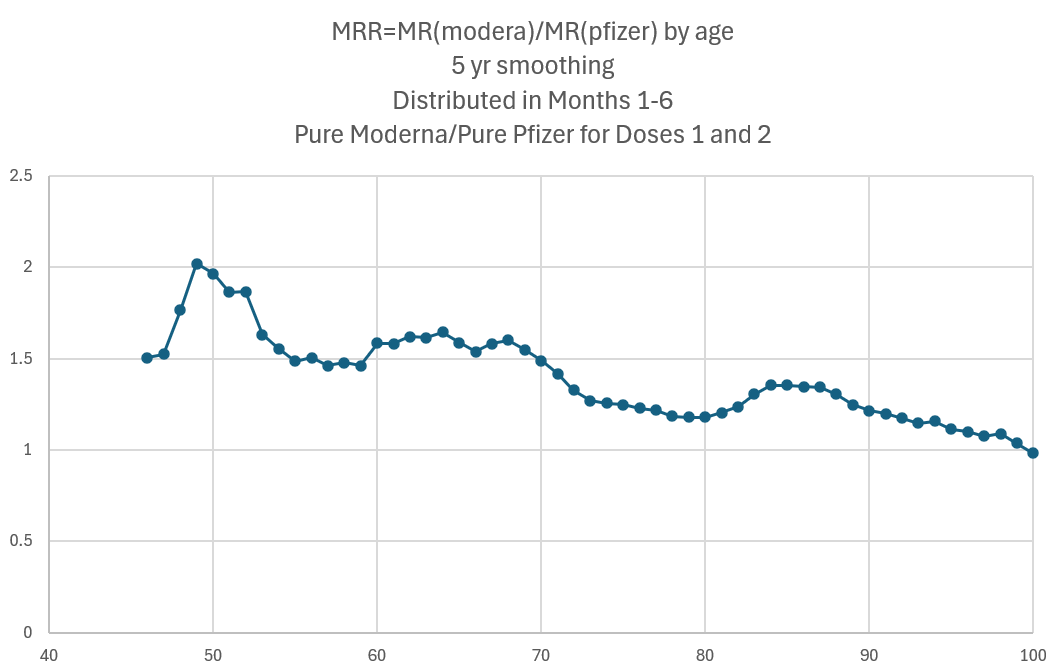
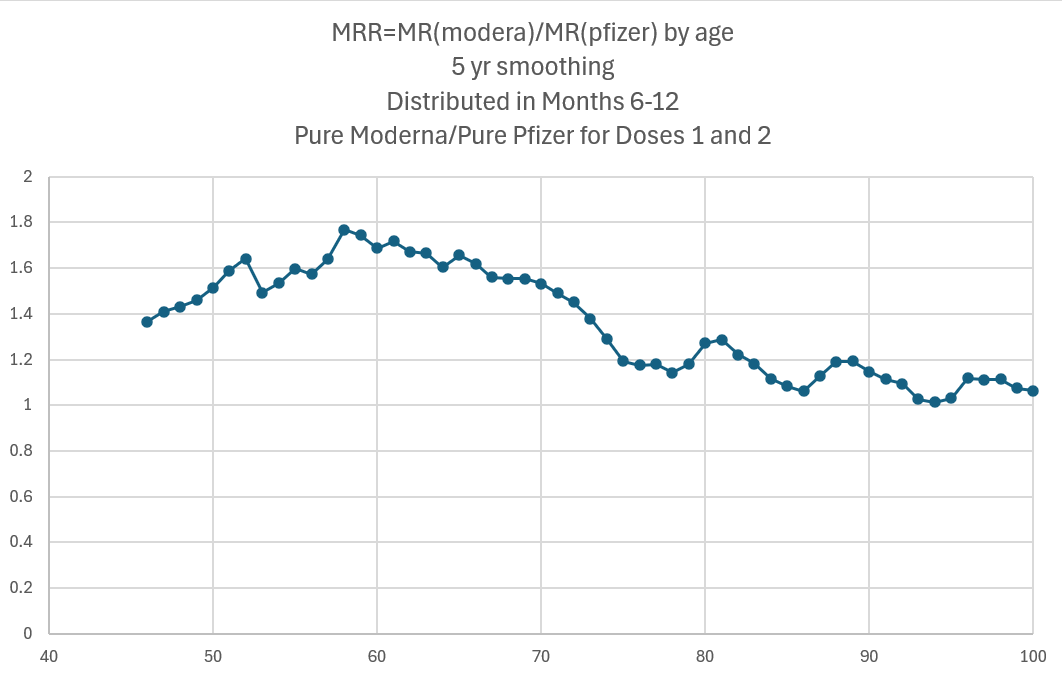
Finally, to eliminate the objection that Moderna vaccines were distributed out over time more evenly than Pfizer, I computed the MRR curves for those who were vaccinated in months 3, 4, 5, and 6 which were the 4 months with the greatest number of Moderna doses. The results are even worse for Moderna.
Consistency across month of vaccination
If distribution biases explained the effect and both vaccines were equally safe, we’d expect that half the months would have Pfizer safer than Moderna and half the months would have the opposite. And we’d expect the differences to be small.
That wasn’t the case.
The results were very consistent across months.
For example, if you were born in the 1950’s and you were brand consistent and got your first shot in 2021, Moderna was more dangerous in 12 out the 12 months (date of first vaccination).
The time series data
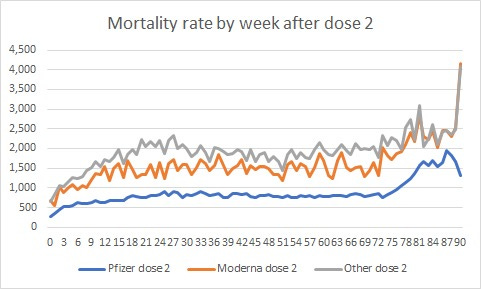
Here is the time series cohort analysis for Pfizer, Moderna, and for the other vaccines (AstraZeneca, Janssen, etc.) lumped as “other” for those aged 40 to 79.
This shows the mortality rate (deaths per 100,000 person-years) by week after the shot is given. Pfizer has the lowest MR, meaning it is the safest. The other vaccines (gray line) had higher mortality than Moderna at nearly every point in time.
The first 3 weeks should be ignored as that is due to the temporal HVE effect (primarily caused by the fact that we don’t generally vaccinate people in hospitals and hospice).
The monotonic rise in mortality for ~25 weeks from the time of the shot is extremely problematic and is seen in other countries using the COVID vaccines. This is not present in other vaccines administered to elderly populations.
Novavax
When Pfizer is compared against Novavax, all illusions of safety go away.
While the Czech Republic had limited use of Novavax, the results are quite stunning in comparison to Pfizer.
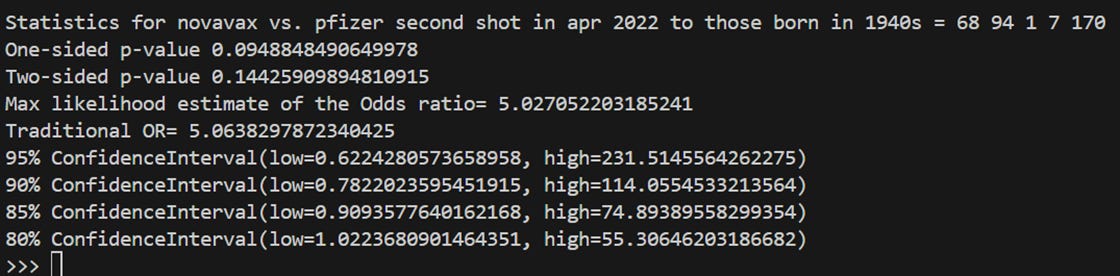
Novavax was not administered in 2021 because it wasn’t available in the Czech Republic until March 2022. Novavax doesn’t appear in the analyses above because nobody would have at least 12 months to die. But we can look at people who got Novavax (CO07 in the original datafile). There were only 6,087 people who got Novavax in total. The month with the most doses was April 2022.
As you can see by looking at the Novavax.xlsx spreadsheet, we can say with 80% confidence that Novavax is likely safer than Pfizer. The ratios are high and consistent, but we need more data to make a more confident assessment. The MRR ratio should be 1 for a safe vaccine.
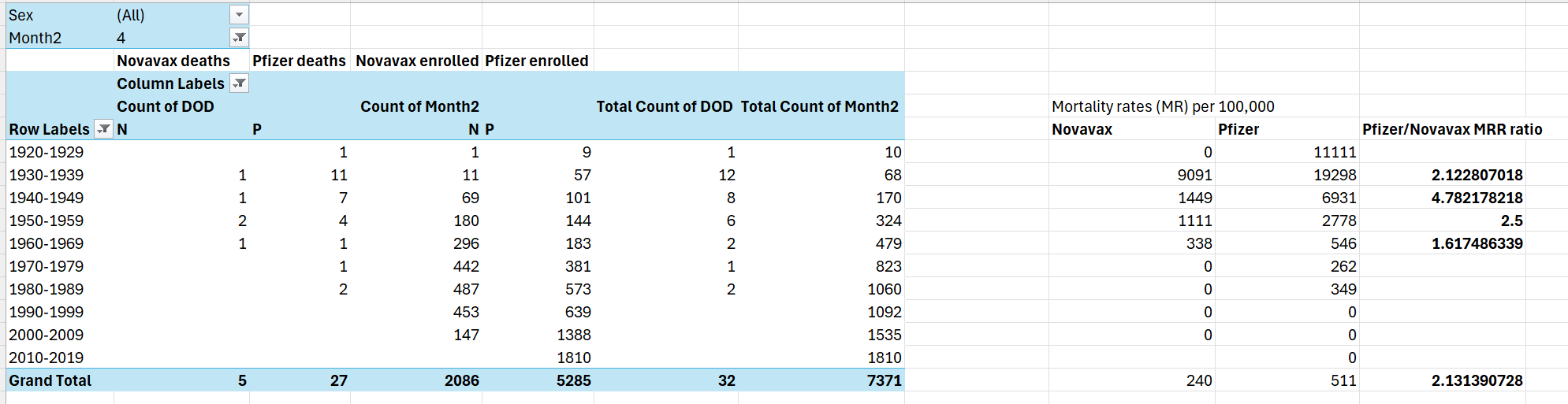
But these numbers 2.1, 4.7, 2.5, 1.6, and 2.1 are far from safe showing that Novavax is highly likely to be significantly safer than Pfizer.
If the Novavax and Pfizer vaccines were equally safe, we’d expect Pfizer to win on half the ratios. But Novavax won on all 5 ratios we had adequate data for.
The change that would happen if both vaccines are safe is just 3% of the time.
Which means it’s far more likely than not that Novavax is far safer than Pfizer.
How did the other vaccine brands do?
To eliminate age confounding, here’s the data for those born in the 1950’s who got their first shot in 2021.
As you can see, of the top 4 brands, Pfizer is the least deadly of the four major brands.
The interpretation of the data
Moderna kills more people than Pfizer. It’s over 50% for ages 46-69.
Pfizer consistently kills more people than Novavax. The data is too sparse to make a definitive assessment, but it’s very highly likely that it is at least 20% or more.
Because those who were most adversely affected were so young, this is staggering in terms of potential man years lost .
For ages below age 46, the number of Moderna shots/deaths to compute accurate ratios diminishes.
Even if Pfizer was 100% safe, Moderna is too unsafe to be used. Remember: this is a ratio of ACM, not a ratio of excess mortality. Big difference. A 50% higher ACM is a train wreck. Vaccines are supposed to reduce ACM, not increase it by 50%.
The highest MRR values were for those under 71. This suggests that the absolute mortality increases caused by the shots are likely relatively independent of age. This explains why we see less of an effect for older people because their absolute MR is very high so that the vaccine mortality is a smaller percentage of their overall all-cause mortality so there is less of a difference on a percentage basis.
These differences cannot be explained by greater vaccine efficacy against death. Even if Pfizer was 100% effective against death and Moderna was 0% effective, the greatest arguable effect size would be less than a 12% difference for those under age 54.
Furthermore, even if 100% of the effect could be explained by differences in efficacy, why would a country choose to distribute a vaccine with a zero death benefit when there is an alternative with a 100% death benefit?
So even if you don’t believe the vaccine killed people, the mortality differential alone should be sufficient to halt the use of Moderna as an ineffective drug even at over 3X the dose of Pfizer.
Correlation or causality?
There are 5 Bradford Hill tests for causality for vaccines.
All five are satisfied:
Consistency: In every single one of 40 different single-year age ranges studied, Moderna had worse mortality. And the Moderna trials had substantial serious adverse events that we are just now learning about thanks to Aaron Siri.
Strength of association: A 50% increase in mortality over 1 year is considered very strong.
Specificity: The Moderna branded vaccine consistently had a mortality rate higher than Pfizer, but less than the other vaccines as you can see from the time-series plot above.
Temporal relation: The increase in mortality began immediately after the shots. The unvaccinated before the shots did not exhibit any increase in mortality.
Biological plausibility: Moderna was over 1.5X the active ingredient than Pfizer. See the section on biological plausibility and more.
Check out this article which combines several of the needed criteria into 2 paragraphs:
A study co-authored by Dr. Peter McCullough found that there was a 1,236% increase in death in King County, Washington between 2020 and 2023. The county had a vaccination rate of 98% of its residents received at least one Covid injection by 2023. The report stated that excess cardiopulmonary arrest deaths were estimated to have increased by 1,236% from 2020 to 2023, rising from 11 excess deaths in 2020 to 147 excess deaths in 2023.
The Covid shots are also known to increase in lethality after repeated doses, increase Covid infection rates, result in turbo cancers, reproductive destruction, cause miscarriages, paralysis, autoimmune disorders in the thyroid, as well as deadly headaches, seizures and heart inflammation. The shots contain hundreds of times the allowable levels of DNA contamination leading to mutagenic effects, as well as likely permanently altering the DNA of the vaccinated and their offspring.
Public health recommendation in light of this data
Unless the drug makers can explain to the world how this new data from the Czech Republic actually proves that all their vaccines are equally safe, the Pfizer, Moderna, Janssen, and AstraZeneca vaccines should be immediately halted as too unsafe to use.
Could the difference between Moderna and Pfizer be explained by vaccine distribution bias?
That could explain the MR differences, but it doesn’t align with the facts:
There was no evidence of distribution brand bias based on number of comorbidities
If there was distribution brand bias based on comorbidities, it would have to be very well organized to get such high odds
The MRR curves calculated in the first and second half of 2021 were very similar. If this was a just distribution bad luck, it’s unlikely the two halves of the year would be so similar
Moderna was between the MR curves for Pfizer and the other vaccines over the entire time in the time series. If this was a distribution bias, it would have had to be executed with surgical precision.
Moderna was between the MR curve by ages as well. So the distribution would not only have had to be extremely consistent every month, but for every age.
The slope of the time series MR curve goes up for 20 weeks then is flat. That is not caused by higher comorbidities. That is an increasing MR that happens at the time of the shot and is ephemeral. If it were just comorbidity bias, we see a series of nearly horizontal lines. There is no such thing as a comorbidity that stops for every older age group at around 20 weeks from the time of a “placebo” shot. We saw the same 20 weeks in other countries as well. The rise for 20 weeks is not HVE since it doesn’t happen with other vaccines given to the elderly.
As there were no indication criteria favoring one mRNA vaccine over the other, we can assume that the vaccines were assigned by convenience (availability at the time at a particular place), providing as random distribution as possible in a population-wide dataset, removing the majority of biases.
We verified that by looking at the the MRR curve for the first half of the rollout compared to the last half of the rollout and the MRR curves were similar:
To achieve odds ratios close to 2 in practice, every vaccinator in the country would have to have had an instruction sheet that told the vaccinator to assess every comorbidity of each patient and if was above a set threshold that would have to vary by age, they were to give them the Moderna shot. There was no such program anywhere in the country that we were aware of.
Biological plausibility
The active ingredient in both vaccines is mRNA. In Pfizer, there is 30 mcg/dose. Moderna is 100 mcg/dose.
So should we be surprised that a 3X higher active ingredient caused a 50% higher mortality rate? No, not at all.
We also have to show biological plausibility that mRNA vaccines can impact death.
Check out this article.
Here are some more examples, but there are millions of stories like these. Dead people don’t post, but here are injured alive people who nearly died as well as just one example of mRNA shots making it more likely for you to die from Dr. George Fareed.



The adverse event rates measured in the gold-standard randomized trials is also consistent with what the Czech data says
The Fraiman paper re-analyzed the gold-standard randomized control trials and analyzed the adverse events. They found that Moderna had a 50% higher rate of serious adverse events of special interest (AESI) than Pfizer vs their respective placebos (15.1/10.1):

So should we be surprised that Moderna had nearly 50% higher all-cause mortality? No. Nobody I asked was surprised.
The VAERS data also is consistent with the Czech data and shows Moderna causes 30% more deaths than Pfizer on a per shot basis
See VAERS data shows Moderna causes 30% more deaths per dose than Pfizer.
The US insurance company data is also consistent with the Czech data
And you will also need to explain why younger people have huge increases in mortality in Q3 2021 right after the shots were required by employers in 2021 that has NEVER BEEN EXPLAINED.

From ChatGPT:
Hmmm…. if it wasn’t the vaccine, what caused such a massive spike in insured working age people? Nobody seems to be able to explain that one. They’ve had over 2 years to figure it out, but it’s still a mystery.
Professor Morris writes: “your insurance data discussion ignores the delta surge” so OK, I’ll include that.
From Gemini (just to be objective about it): “That said, general trends suggest that the IFR for the Delta variant was lower than previous variants, particularly for younger age groups. This is likely due to a combination of factors, including increased immunity from previous infections or vaccinations, and improved medical treatments.
But the more important thing is this key sentence from this article: “Most of the claims for deaths being filed are not classified as COVID-19 deaths, Davison said.”
So, if most of the deaths aren’t from COVID, what are they from?
p-value calculation
These results are highly statistically significant, especially for older age groups where there are many deaths.
Here is the Fisher Exact test for ages 65-69 showing those who got the Moderna shot #1 in 2021 has a most likely 1.6X higher odds of dying compared to those taking the first Pfizer shot.
Statistics for pfizer vs. moderna study1 ages 65-69 = 408457 39439 3463 534 451893
One-sided p-value 1.827603389620981e-21
Two-sided p-value 2.764503609787533e-21
Odds ratio= 1.5970138080953098
95% ConfidenceInterval(low=1.4543479879419918, high=1.7509540207812164)The low p-value means that there is no chance that the groups are the same, and with 95% confidence, the true odds ratio Moderna:Pfizer is between 1.45 and 1.75.
Note: Moderna odds of dying is defined as # dead: # remaining alive at the end of the 1 year period.
Even if Pfizer was completely safe (which it isn’t which I’ll show later), Moderna is an unsafe vaccine.
Third party analyses
Dr. Clare Craig
One of the many plots she’s produced shows just how dramatically different the different brands affected young people.
She wrote, “20-29 year olds did really badly. Here I have taken the cumulative deaths in a standard population and plotted the Pfizer deaths as a percentage of the total Moderna deaths.”
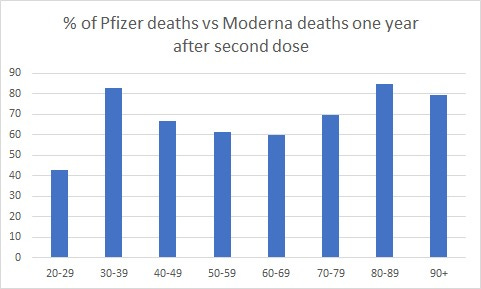
So Moderna killed over twice as many young people than Pfizer did on a per shot basis.
We tried to warn people that COVID vaccine mandates were a really bad idea since students rarely die from COVID. But none of the world’s health authorities and none of the medical community would listen.
For example, in mid-2021, I had a call (along with Robert Malone and other scientists) with Stanford University Dean of Medicine Lloyd Minor and some of his staff members to warn them of the dangers of these shots. They sat there, didn’t ask any questions, and then at the end said, in essence, “Thank you for sharing. We are not interested in engaging with you in the future. Have a nice day.”
Universities mandated these shots and failed to warn students about the huge mortality differences between shots. They weren’t interested in seeing the data; they simply had blind trust in the CDC and FDA and if you had a different point of view, you weren’t worth listening to. That blind trust cost students and faculty members their lives. No apologies.
Professional epidemiologist
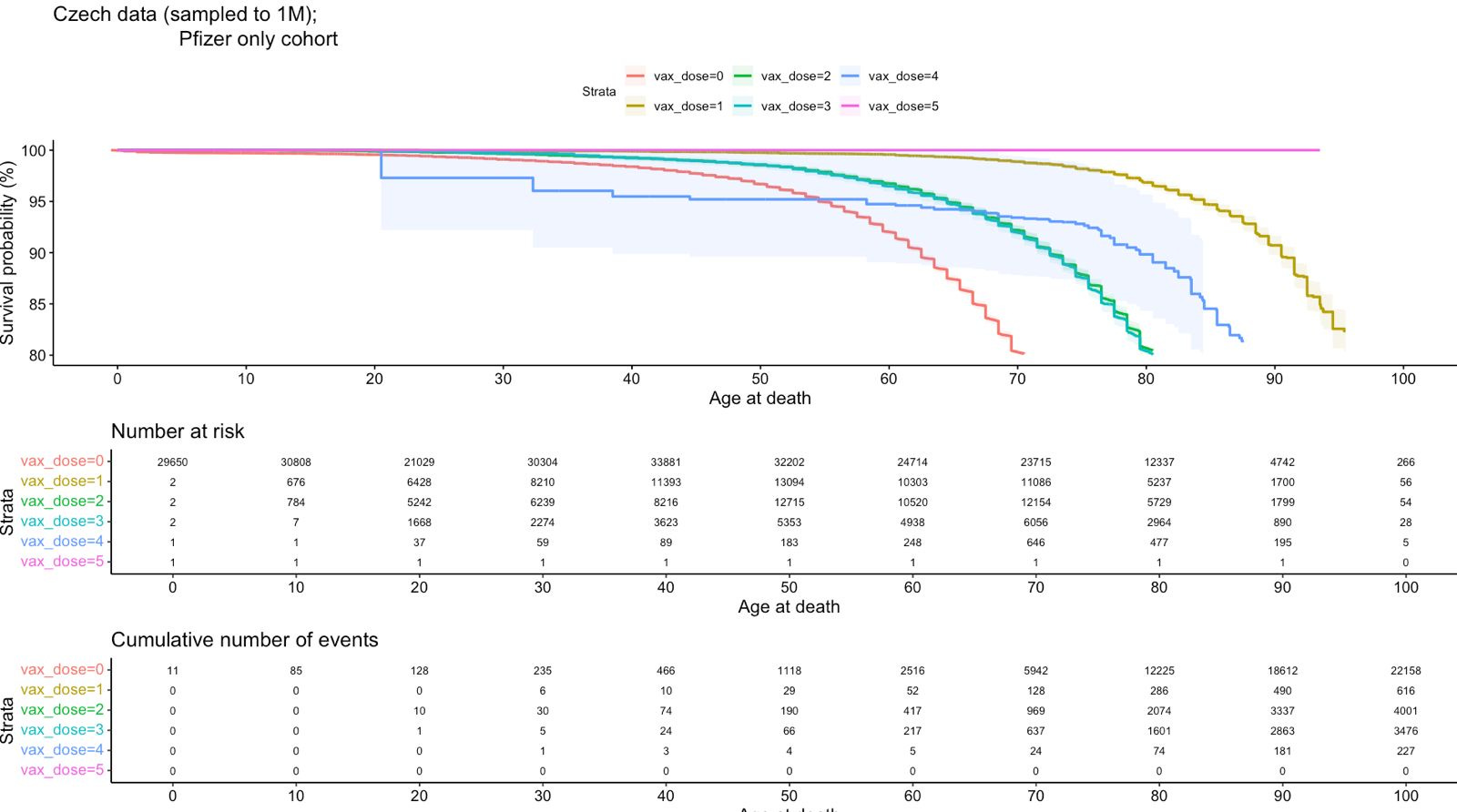
From an epidemiologist who fears for his job if his name is associated with anything that isn’t consistent with the government narrative are these survival analysis plots. I’ve posted his R source code to my github repo (in ./code/survival analysis.R) to protect his identity so you can verify the graphs. He had limited RAM in his system so he did this on a random sample of 1M records.
The first plot is a survival analysis for Pfizer for the different doses. Since subsequent doses had less time to die, these should all be right shifted from dose 1 if the vaccine is safe. As you can see, dose 1 has the most right shift which is extremely problematic if there isn’t a bug in the code. Note in the table, it’s a cumulative number of events which is why the number of events is highest in the 100 column.
Here’s another survival analysis comparing unvaccinated, Pfizer, and Moderna. Everyone should always be to the right of the unvaccinated line because the unvaccinated are undercounted so their mortality is always super high in comparison to any vaccinated group. So it is extremely problematic that Moderna shot 1 is to the left of the unvaccinated. And Pfizer shot 2 and Moderna shot 3 are nearly on top of each other when they should have horizontal separation, confirming once again that Moderna is far more dangerous than Pfizer.
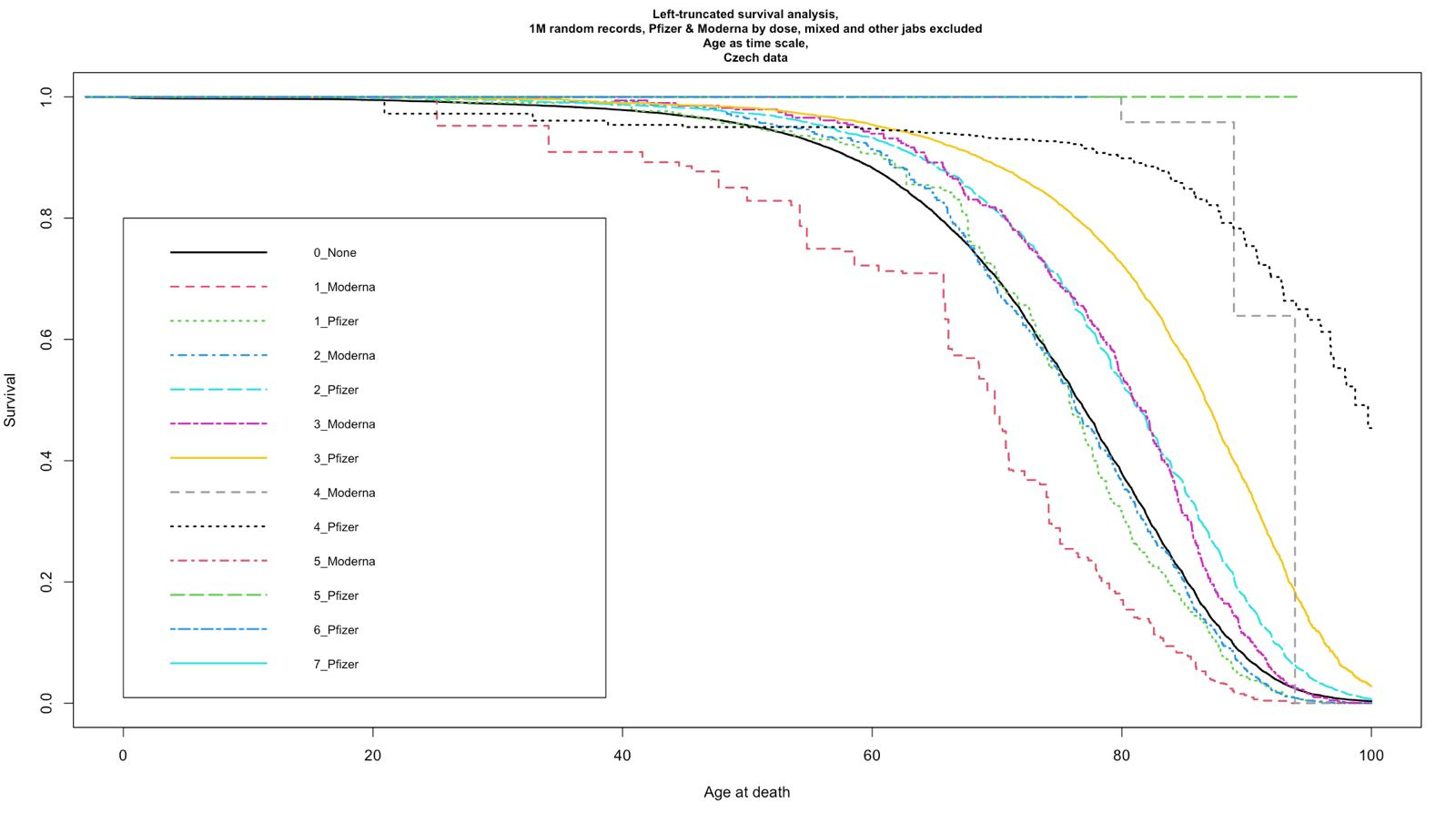
CAVEAT: I just got these plots and they have NOT been independently replicated by others.
Henjin
Henjin’s analyses can be found on his web page for the Czech data.
The best single graph that tell you everything you need to know is here:
This shows that the mortality difference between Pfizer (blue) and Moderna (red) was present in times of high COVID and no COVID. This is a disaster for the vaccines since there should be no difference between brands during high COVID periods vs. no COVID periods if the brands are all safe and the differences are due to effectiveness in preventing all-cause mortality.
Furthermore, if the brands have different efficacy in preventing COVID mortality, we’d see the “gap” between Pfizer and Moderna consistently widen or narrow depending on whether Pfizer is better (widen) or Moderna (narrow) is relatively better in preventing death from COVID. The gap remains within the boundaries established in the low COVID periods: so neither vaccine was any better (if at all) in lowering COVID ACM (if in fact they lowered ACM). No difference in COVID protection between brands.
The single most troubling thing is the minimum mortality in 2021 for both brands is lower in 2021 than 2022. How is that possible? It’s only possible if both vaccines increased ACM. Was this a background effect? Nope, because the “unhealthy” unvaxxed had lower mortality in 2022. This should cause alarm bells to be going off everywhere. We goofed!!!
Also, in periods of high COVID, we should see the mortality gap between each of the vaccines vs. the unvaccinated widen in peak COVID periods and then narrow back to what it was during non-COVID periods and there should be consistency in this every time there is a COVID wave.
What happens? The mortality gap goes the other way: it NARROWS during COVID periods which means that the COVID vaccines made it MORE likely for you to die from COVID, no less likely.
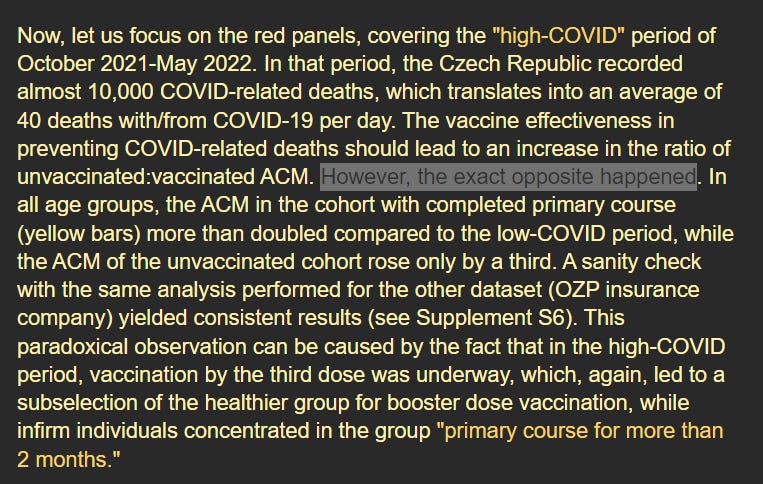
Henjin is honest enough to point that out where he notes “the exact opposite happened” as you can see from the chart he provides below:
Then he follows that with a hand waving explanation that that’s because nearly everyone who was healthy ditched the cohort to get the next booster shot. But he provides us with no evidence whatsoever that his speculation is correct.
He admitted during COVID times, the unvaccinated had a 1/3 increase in mortality, but mortality doubled in the vaccinated groups. Was this really caused by group migration to a 3 dose group?
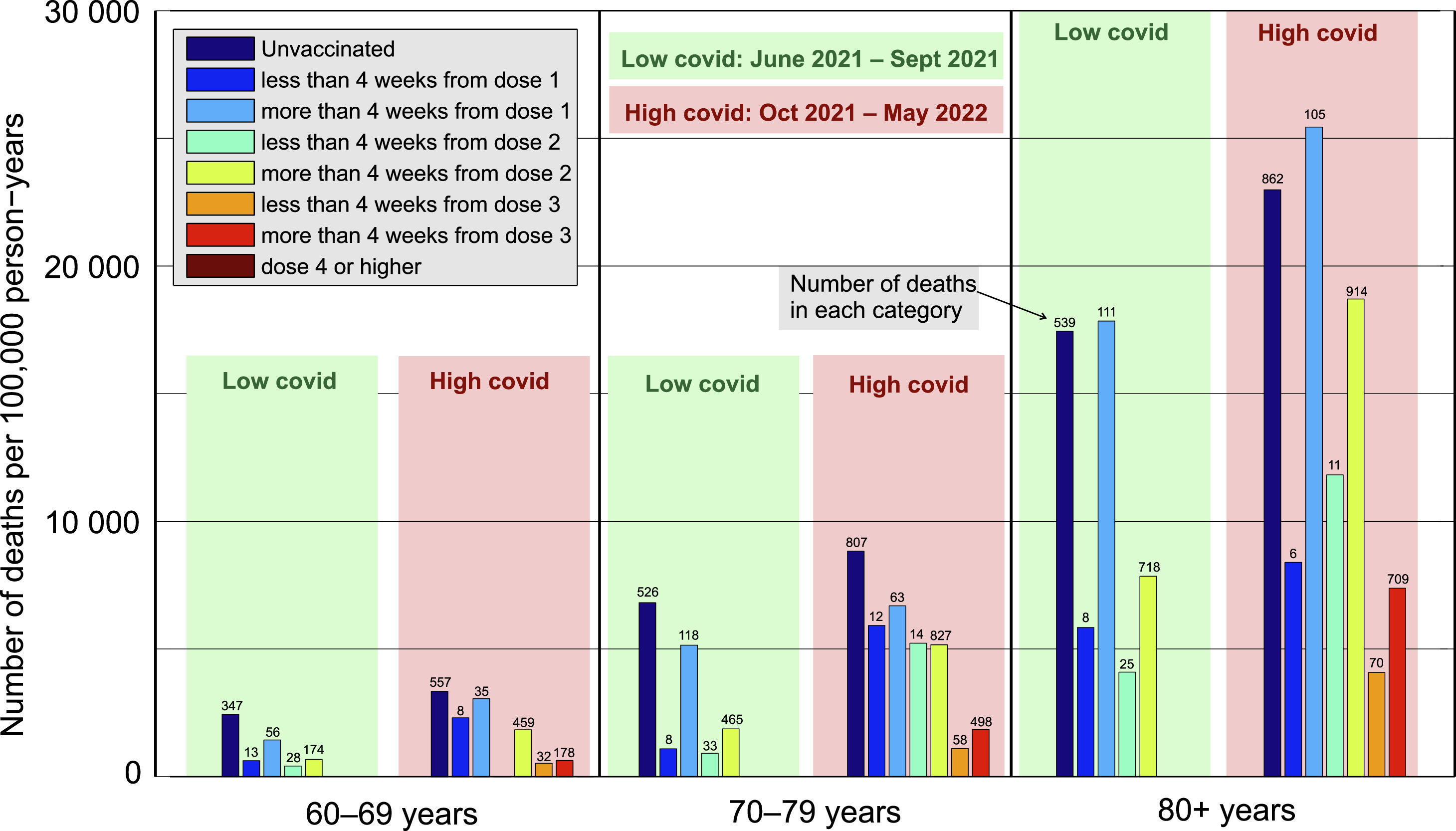
He shows the MR by the height of the bar, but he also notes the actual death counts in each cohort at the top of each bar. That was clever! Now we can just do some manual calculations to see if he’s right. We simply look at the absolute death counts using the numbers at the top of each bar.
We have for ages 70-79 for example:
Low COVID U/V: 526/(8+118+33+465) = .84
High COVID U/V: 807/(12+63+14+827+58+498)= .54
At first glance, this looks like a disaster for the vaccinated because if the vaccine lowered mortality, it should have gone the other way.
However, the overall ratio in terms of number of people in the unvaxxed vs. vaxxed group changed between the periods, so you can’t just compare ratios like that. You have to adjust for the fact that the U/V people count ratio changed between those two time periods which reduces the differential.
In regards to his time series analysis, note that the epidemiologist who did the survival analysis says that Henjin’s survival analysis “is quite different to what I have done.... not time varying covariates.... not standard survival analysis.”
Here are the Pfizer vs. Moderna curves from Henjin for the different doses. If both vaccines are safe, these should be on top of each other.
What’s impossible to see from Henjin’s plots below is the HUGE difference for younger people because the absolute numbers are so small, but the percentage differences are huge.
This is a perfect example of why you always rely on multiple ways to look at the differences.
Implications
This data means it’s time for the medical community to face reality: they fucked up big time with their willful blindness and 100% trust in the CDC and FDA. Nobody wanted to see any data. Nobody was asking for data transparency.
These people need to face the music: they were wrong. They need to admit it and demand data transparency moving forward.
The longer they resist accepting the truth, the worse they look.
The first rule of holes is when you find yourself in one, stop digging.
Unless the world’s health authorities currently possess better data than I do that shows I’m wrong, they should do the right thing now and suspend the use of Pfizer and Moderna.
And if they claim they have the data showing I’m wrong, they need to show it and make it public just like I did so the public can discover who is telling the truth and who is not. After all, we all agree that misinformation is a bad thing, don’t we?
Why aren’t we just comparing the vaccinated mortality with the unvaccinated mortality like all the other studies do?
Because in most countries, the unvaccinated are hard to count (until they die). This makes it appear that the unvaccinated die at a substantially higher rate than the vaccinated. Using the unvaccinated as a comparison group can create a “mirage” that the COVID vaccines saved lives! Other factors such as the “healthy vaccinee effect” (HVE) also impact the comparison (see for example Does the healthy vaccinee bias rule them all? Association of COVID-19 vaccination status and all-cause mortality from an analysis of data from 2.2 million individual health records).
I wrote a Substack on this early on: FDA discovers fountain of youth where a study passed peer-review and showed an impossibly large reduction in all-cause mortality after they got the shot. The medical community keeps repeating this flawed methodology over and over because it fits their narrative. It’s fraudulent.
This is why this new methodology where we compare vaccine brands with each other is so important. EVERYTHING is identical about the recipients EXCEPT the brand they were given. This is known as convenience sampling.
No official guidelines have been published in the Czech Republic that would have skewed the choice of vaccine administered to a person based upon the number of their comorbidities.
You’ll find that there is a huge range of mortalities for a given age because people who choose to be vaccinated can easily have half the mortality of those listed in the official Czech Republic mortality data. The vaccine didn’t save lives… it was just the people who opted for vaccination are not in hospice, sick, or dying, so the mortality rates are stunningly lower than the rates listed in the mortality tables.
Attack vectors
Like any piece of science, this work can be attacked from four different angles:
The data
The methodology
The data extraction tools (e.g., code error)
Interpretation of the results of the methodology
There are various hand waving attacks that people have tried to use to explain this data.
The key thing is you simply need to explain a more plausible hypothesis that explains all the observed data mentioned in this article.
For example, one person said that the average age was different between the groups. This is expected because the rollouts were by age and depended on which vaccines were most available at the time the person decided to get the shot. But this does NOT create bias based on comorbidities; it creates biases on age distribution. To avoid this bias, we analyze based on 5 year age ranges. Also, the data itself can be analyzed by single age ranges and the same effect is observed.
The most plausible argument is that Moderna and the other vaccines were given exclusively for people with high numbers of comorbidities in every age range. There is no evidence whatsoever that this is the case. Nor was there any program to instruct vaccinators to ask the patients how many comorbidities they had and then assign them a vaccine based on the comorbidities.
The differences in mortality between the brands cannot be explained by vaccine efficacy. Even a 100% difference in the vaccine efficacy could not have led to the huge observed difference in the ACM. The John Ioannidis paper, Age-stratified infection fatality rate of COVID-19 in the non-elderly population, say that “the median IFR was 0.0003% at 0-19 years, 0.002% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.123% at 50-59 years, and 0.506% at 60-69 years.” And the data from the Czech Statistical Office doesn’t support a 50% mortality difference either. So good luck making that argument stick. The numbers cannot possibly work out. You can explain a 1% difference maybe, but a 50% difference?? No way.
Infection fatality rate of COVID-19 in community-dwelling elderly populations, says “Median IFR in all elderly for all 11 high-income countries was 4.5% (range 2.5–16.7%).” That means Pfizer cannot reduce ACM by more than around 4.5% at best, even if everyone is infected. And in those
I didn’t find any errors in the Czech data. That’s very rare. They did an excellent job of data entry and validation. The records supplied align with the official Czech Republic statistics.
I don’t believe that the methodology can be attacked. It doesn’t get any simpler than this. The computer code was simple to write and easy to verify. You just count the number of people vaccinated with each brand in a month, you count the number of deaths within 1 year of vaccination, and you divide the results. To avoid confounding by age and month of vaccination, we analyzed the data by month and by birth year and you get similar results.
The interpretation is as straightforward as it gets.
The bottom line is we are open to being shown we are wrong, but to do that, you must demonstrate the “correct” way to analyze the data and show that the data shows that it is more likely than not that Pfizer and Moderna both being equally safe.
There are those who claim 95% of the people who die from COVID are not fully vaccinated
So why aren’t they making the record level data public on that? Why does it have to be a secret?
Here’s the secret…
The way they arrange to make these magical statistics happen is by using hospital data. By default, in many hospital systems, by default you are unvaccinated (rather than unknown) and systems like EPIC can make it very hard for hospital staff to change this. See how this can change the data? Everyone who dies is magically unvaccinated.
The other problem with this argument is that ACM rules everything at the end of the day. If you give a vaccine and the ACM decreases, that’s good. If you have an ACM that is even 10% higher than your competitor at ages under 65, you have a vaccine that is greatly increasing people’s net risk of death even if it was 100% successful in preventing COVID deaths.
These vaccines were NEVER better for the elderly or anyone else
These shots increased the risk of getting COVID, resulted in no COVID hospitalization or COVID mortality benefit, and increased all-cause mortality.
They shouldn’t have been approved and they never should have been mandated.
The shots were designed to reduce mortality in the elderly which is where most of the deaths were happening.
Think about it… if the shots worked in the elderly, there would be a huge signal in the US Nursing home data (15,000 nursing homes) after the shots were rolled out and there would be papers published in the literature showing this data proves the vaccines are safe and effective. No papers. So you don’t have to go any further than that, do you?
Here are my favorite 4 arguments that the COVID vaccines had no COVID mortality benefit:
The US Nursing home data is the ground zero dataset for showing the COVID vaccine reduced deaths from COVID. It doesn’t get any better than this dataset. But the funny thing is that there isn’t a single paper published showing how this gold-standard data proved the vaccine saved lives! How is that possible? Easy. The data showed the opposite! In fact, after 60% of the nursing homes were fully vaccinated, the COVID CFR was over 50% higher than it was at the start of the vaccine rollout! That’s why there is no paper. And no paper on this data means they lied to you about the vaccine saving lives. It didn’t save lives at all. If I showed you the data and asked you to tell me when the vaccine rolled out just by looking at the data, you’d never be able to do it. Because their own data didn’t support their promises, they completely avoided talking about it.
The VA study in JAMA also shows no hospitalization benefit at all. Zero. Zip. The author can’t explain it. So when you see stuff like this clip, you need to know the the gold-standard VA evidence does NOT support the claims at all:
Apple Valley Village, for example, averaged one all-cause death/week before the shots, and then averaged 8/week for 3 weeks right after the shots rolled out. That’s an 8X increase in the weekly death rate after the shots rolled out. They don’t want to talk about it and the police refuse to investigate.
Tidewater Family practice, a geriatric medical practice went from 8 to 10 deaths a year before the vaccine to 48 deaths in 2023. They attributed the rise in all-cause mortality to the COVID vaccine. How is that even possible if the vaccine saved lives? Where is the success story where when they rolled out the COVID vaccines that both all-cause mortality as well as death rates from COVID dropped by 10%? It doesn’t seem to exist, although people think it must. AFAI
K, there is no success story.

A bit more on the VA study…
This carefully done VA study showed the COVID vaccine didn’t reduce hospitalization at all. Zero. Zip. Nada.
And how can a vaccine which provides no hospitalization benefit provide a death benefit? Nobody can answer that.
I asked the author to explain how the vaccine breakdown in both cohorts were identical if either vaccine works. He couldn’t. And then he stopped answering any of my other questions.
I guess it’s not OK to ask questions in science nowadays.
The bottom line is why are we pushing a vaccine when after 3.5 years we can’t even name a single nursing home that is a success model? Look, if even 5 out of 10 nursing homes reported lower COVID mortality AND lower ACM post COVID shots, I’d be impressed. Where are the success stories? I tried to talk to nursing homes and they didn’t want to say anything.
We and of course, we have plenty of stories of harm that are unprecedented like this one I just got. These are not “coincidences.” I’ve never seen so many stories like this one for any vaccine ever.

Google’s AI agreed with me: my methodology is sound and the MRR should be very close to 1 if both vaccines are safe
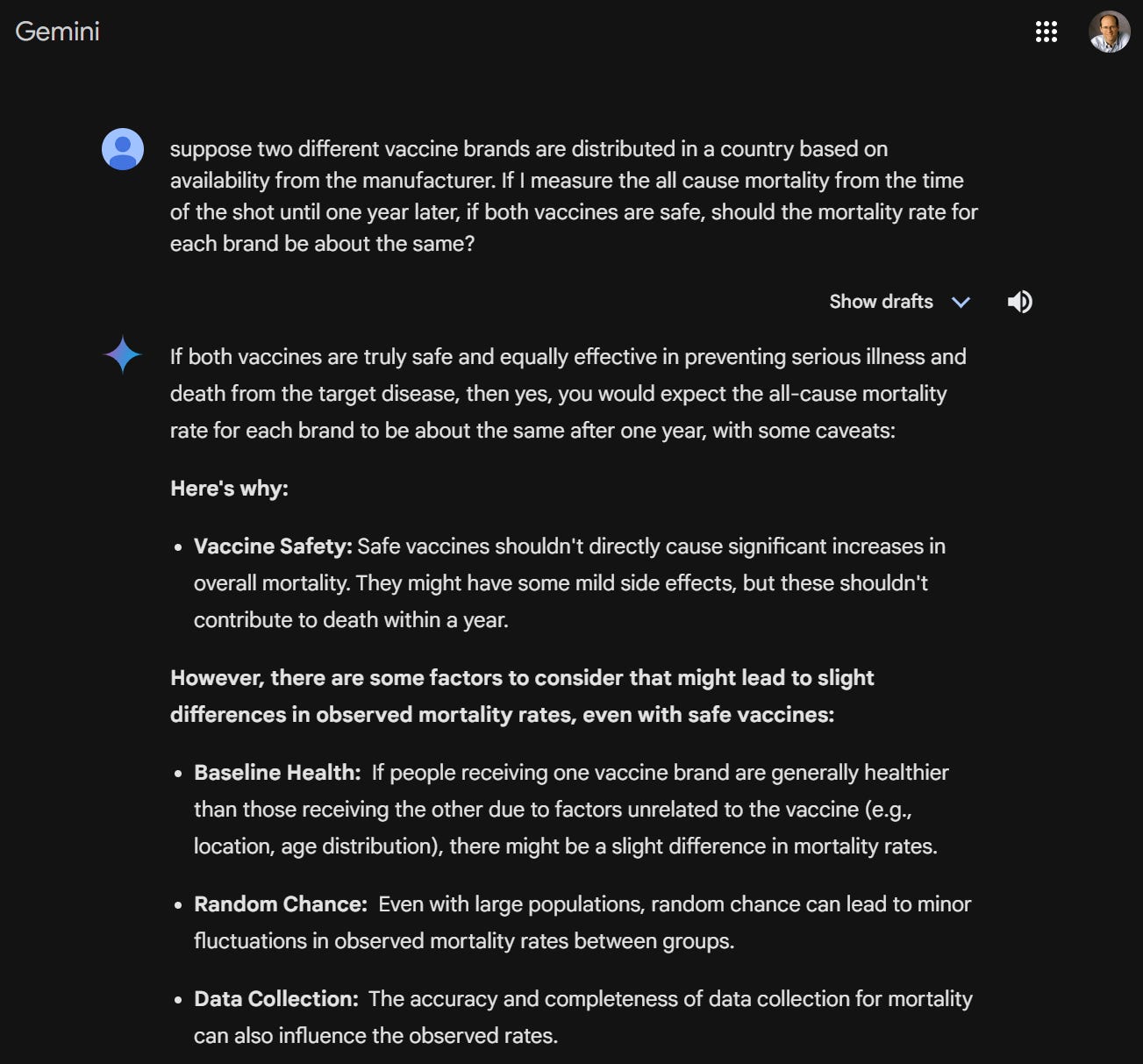
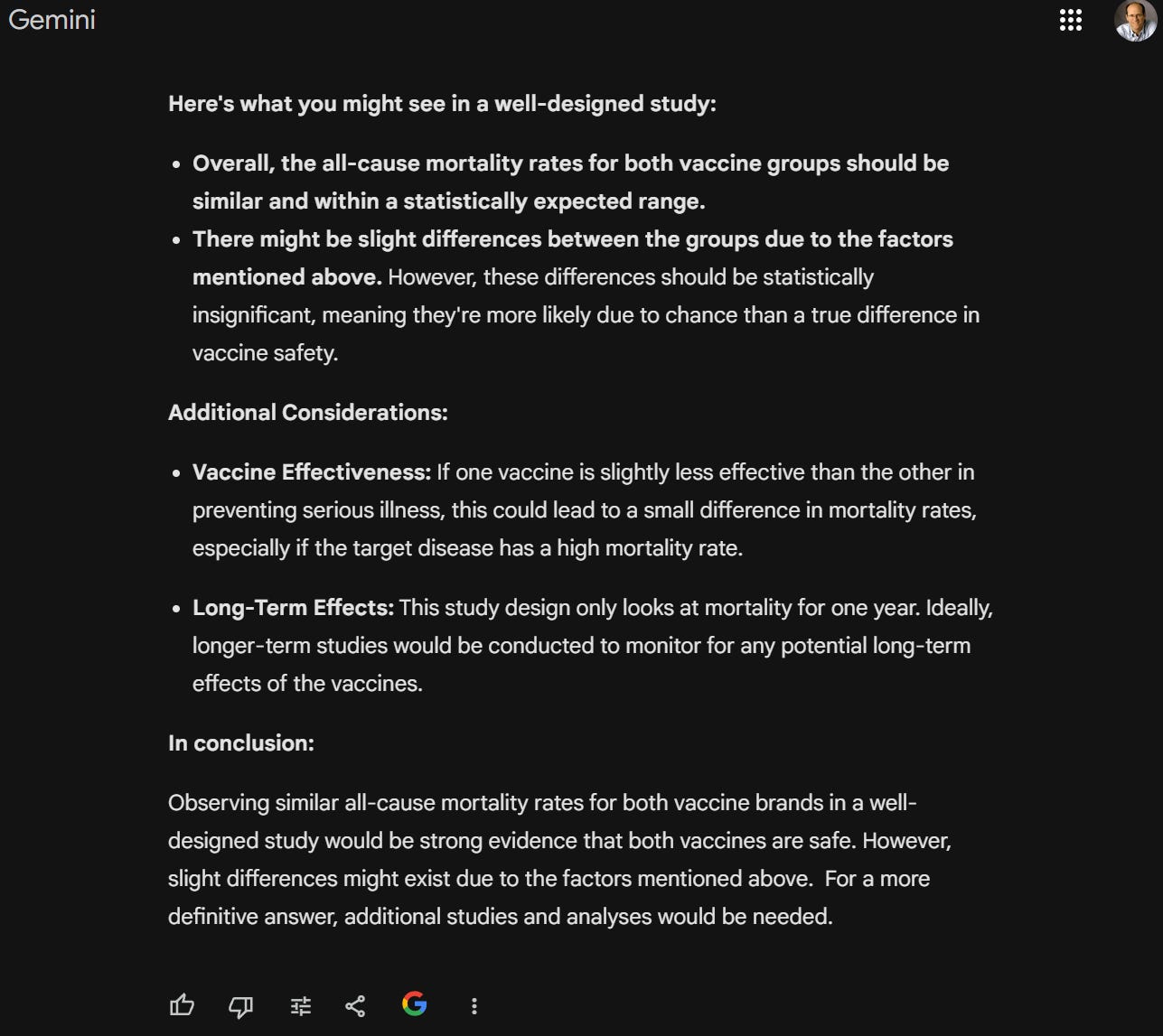
I agree! Slight differences (on the order of 1% for those under 69 years old) would be expected. But a 50% difference that is statistically significant is not a “slight difference.”
Critical thinkers would ask, “If the vaccines are so safe, why isn’t any health authority in the world releasing the data publicly like the Czech Republic did???”
This is exactly the type of data that any honest public health authority should be making publicly available so that anyone can ascertain whether vaccines are safe using the SAME data.

Unfortunately, no public health agency on Earth has ever willingly made this information publicly available. Apparently, they all believe that keeping people in the dark about vaccine harms leads to better health outcomes. I’m joking. They don’t want to make the data available because they don’t want anyone to know that their recommendations killed people.
I don’t know of a single member of the mainstream medical community calling for this basic level of transparency. Not a single one. I’d love to ask them why, but they don’t want to answer any questions.
So that alone should tell you everything you need to know about this data. The medical community hates data like this because it reveals the truth. That’s why not a single one of them will call for this data to be produced in their state or country.
Moderna will ignore this data and tell everyone else to ignore it as well. This data sinks their company. If an honest mainstream epidemiologist looked at this data, it would be all over.
I predict that Moderna will ignore this data and refuse to comment. They have to do that because they cannot attack the data or the methods and provide a more plausible explanation.
If nobody can credibly explain how the Czech Republic data is consistent with a safe vaccine, and Moderna itself refuses to explain the data, health officials should immediately remove Moderna from the market.
At a minimum, the precautionary principle of medicine requires that the medical community make everyone aware that it is highly likely that Moderna isn’t as safe as they thought it was.
If I got it wrong, show us the mistake. If you can’t show us the mistake, then you need to accept the result. Refusing to look at the data is not acceptable.
Pfizer isn’t safe either
Pfizer isn’t safe.
Here’s the fastest way to prove this to yourself: if you ask people who have had friends die unexpectedly from the COVID shots, you’ll find that Pfizer is actually mentioned more often than Moderna (because there were fewer Moderna doses delivered into arms in the US). If Pfizer was safe, all your friends dying suddenly would have Moderna in common.
Also, you can never achieve those excess death numbers in Table 5.7 above if Pfizer was perfectly safe and it was just Moderna that was a deadly vaccine. Over half the shots given in America were Pfizer. If Pfizer was safe and Moderna increased ACM by 50%, then at best you could only increase mortality by 25%, and that’s if everyone was vaccinated. See the problem? Pfizer has to have increased the all-cause mortality by at least 25% to explain the data observed by the insurance companies. So Pfizer is a disaster too.
And then there are the “impossible anecdotes” that are 100% independently verifiable. For example, I have one friend (Jay Bonnar) who had 15 friends die unexpectedly after the shots rolled out. He never lost any friends unexpectedly in his life before the jabs rolled out. Get this: 4 of the 15 died on the SAME DAY as their PFIZER JAB and 3 of the 4 were 30 or younger and perfectly healthy.
Jay Bonnar's anecdote is statistically impossible if the COVID vaccines are safe. If the FDA is telling the truth, an event with probability poisson.sf(14, .25)=5.6e-22 just happened to one of my friends. To date, nobody has been able to explain how this can happen. It is “statistically impossible” if the vaccines are safe. I was able to verify each of the deaths through Internet searches. This data is consistent with vaccines that kill people. Academics hate anecdotes like this because they are inconsistent with their studies. But there is only one truth and anecdotes like Jay’s simply have fewer moving parts where something can go wrong.
In Sonoma/Marin, there have been 5 Pfizer vaccine deaths and 0 COVID deaths. This is all verifiable, but no fact checker is going to take that one on. If the Pfizer vaccine is reducing COVID deaths, how can statistics like this ever be observed
And we have the time-series cohort analysis data. The people who opt for vaccination are, in general, healthier than their unvaccinated peers. So if the vaccine is safe, the MR over time should be relatively flat after a short 3 week temporal HVE exponential rise. It’s not flat. This is the smoking gun. It’s not seasonality (which stays flat when it isn’t winter) and it’s not extended temporal HVE. It’s vaccine induced mortality that is getting higher and higher since the time of the shot.
We also have the Pfizer randomized trial data. At no time were deaths in the treatment arm lower than the placebo arm. If the vaccine was perfectly safe, this is not likely to happen.
And last but not least, we have the smoking gun proof with Novavax which significantly bested Pfizer in every age group where there was sufficient data to make a comparison. Whoops!
If Pfizer thinks their vaccine is safe, why aren’t they urging public health authorities worldwide to make the data public?
exactly like the Czech Republic did so they can prove that Pfizer is safe.
But they aren’t doing that. They are saying nothing. What are they so afraid of? That people will learn the truth??
The Czech Republic proved that the data can be publicly disclosed without violating anyone’s privacy (you just supply the YOB instead of the DOB). It’s brain-dead simple.
If the medical community has any doubt whatsoever about these results, they should call for data transparency in every state in the US and every country in the world
But the medical community will remain silent in order to keep their jobs and their medical licenses.
I don’t think a single member of the medical community who supported these vaccines will call for similar data to be made public in their state or country.
Because they don’t want to know the truth and they don’t want you to know the truth either.
Will the FDA and CDC look the other way? Yes.
They will issue statements to the press that they don’t comment on studies that the vaccines have been thoroughly tested and are safe.
And they will say they do not comment on studies that were not done at the FDA or CDC.
And of course, they’ll never look at the Czech data.
It doesn’t matter how many people have to die in the meantime.
Their position is that all the COVID vaccines are safe so why waste time looking at gold-standard evidence that challenges their beliefs when you can just ignore data you don’t like?

How can I be so sure this is right?
For more than 3 years now I’ve been saying the COVID vaccines are unsafe.
Nothing I’ve seen in those 3 years has changed my mind.
Keeping the public health data secret is a huge red flag. If the vaccines were safe, why do you need to hide the data?
I don’t know of a single person who has stated the vaccines are unsafe who has switched to the other side. Can you name one?
But the most important confirmation to me are the anecdotes that I can personally independently verify as true, some of them very close to home. These anecdotes are “statistically impossible” to have happened if the COVID vaccines are safe. Jay Bonnar’s story is a prime example.
When you have the right hypothesis, you can explain the large data and the anecdotes. When the large data and the anecdotes do not align, one of them is wrong, and it’s nearly always the large data and scientific studies.
A safe vaccine
At worst, vaccines should never increase absolute ACM by more than .01% or roughly 1 death per 1M doses. Here’s the reference.
All the COVID vaccines fail this test, except maybe Novavax. We just don’t have enough data on that yet because it’s all kept secret.
The stunning attempt to debunk this analysis written by UPenn Director of the Division of Biostatistics Professor Jeffrey Morris
Here are the two emails he sent me.
In the first email, he attempts to debunk my analysis without even reading it (other than the abstract). He thinks I am doing a total ACM calculation, rather than a calculation for each 1-year wide age group. He throws in a few ad hominem attacks at no extra charge.
In the second email, he’s now clearly read the article, and he realizes now that his earlier email completely mischaracterized what I did and didn’t apply.
So he rattles off 6 defects in what I wrote that have nothing whatsoever to do with the main outcome.
The bottom line is that he admits that he unable to explain why Moderna has a consistently higher MRR if the Moderna vaccine is safe, but he believes there must be a confounder that explains it.
Great! I’m all ears! Let’s hear it!
He says he’ll get back to me.
I wrote him an email urging him to focus on the big picture: what is the confounder explaining why the MRR is higher for Moderna in every single age group where there is sufficient data (there are 40 of them and Moderna loses 40 out of 40).
He is now in a no win situation because to admit the vaccines are unsafe would destroy his credibility.
But as far as we know, there is no way to credibly explain what could produce these results. This is what makes this data and analysis method so powerful.
Therefore, his only option is to stall for time claiming he’s working on it. I predict that is exactly what will happen.
Testimonials

"I am amazed that it took the authorities 4 years to release individual level data. If we had this type of data earlier, we would have been able to avoid the biggest mistakes of the pandemic response. All governments should immediately release this data."
— Tomas Fürst, Data Scientist, Czech Republic
“The patient level data from the Czech Republic is astonishing and very disturbing.”
— Paul Marik, MD
“All Governments hold record level data on their Covid 19 vaccination database. This analysis of the Czech Republic data demonstrates why they won’t release it. These experimental treatments must be withdrawn immediately to prevent further harm to the public.”
— Andrew Bridgen, former MP, British Parliament
“Health authorities worldwide need to explain how this data shows the Moderna vaccines are safe, or they need to ban Moderna.”
— Dr. Aseem Malhotra, MD, Cardiologist (UK)
“It just doesn’t get any more clear than this.”
— Dr. Chris Martenson
“This analysis confirms a “dose-responsiveness” relationship in causing mortality given that Moderna has more mRNA in the vials than Pfizer. Dose responsiveness is a scientific pillar of proving causation. Further, the magnitude of the higher mortality of Moderna recipients compared to Pfizer recipients is consistent with the relative increase in VAERS reports between the two products. There needs to be a moratorium on all mRNA gene therapy products stat. Full Stop. End of story.”
—Pierre Kory, MD
“This analysis is an absolutely stunning treatise regarding the dangerous nature of the Moderna (and Pfizer) shots. You can’t refute these results! And they are wholly consistent with what would be expected given the high dose of mRNA in the Moderna jab. People died needlessly and justice should be served!”
— Brian Hooker, Chief Scientific Officer of Children's Health Defense
“This is a significant observation that should mandate further confirmation urgently.”
— Drew Pinsky, MD (aka Dr. Drew)
“Using Moderna to Pfizer ratios, Steve Kirsch demonstrated that Czech Republic record-level source data provides reasonable belief that COVID vaccines are killing people. Government officials have a legal duty to immediately and earnestly investigate these findings and halt COVID "vaccines" for the safety of their citizens.”
— John Beaudoin, author, The Real CDC
“I don't see any possible way for them to explain this data. It’s devastating. And the methodology is novel and brilliant.”
— Dr. Clare Craig, independent data scientist
Acknowledgments
Dr. Clare Craig worked with me on the analysis to ensure that no mistakes were made. Check out her Substack on our work.
Jaroslav Janošek Ph.D. and Tomáš Furst made me aware that the Czech data has been sitting on the Internet for four months and nobody noticed. They also pointed out potential attack vectors and provided helpful comments on this post. Check out their papers on HVE which explains why papers that claim the COVID shots saved lives are flawed:
Andrew Bridgen first suggested that the results were remarkably consistent with the Fraiman paper.
Dr. Joseph Fraiman tried his best to poke holes in the interpretation of the data. I heard he told someone privately that he thinks this is the best work I’ve ever done.
Unnamed epidemiologists reviewed the data and methodology. I can’t name them because they are afraid of losing their jobs. That’s just how science works nowadays.
If you think public health epidemiologists are looking at the vaccine data, think again
I used to believe that the epidemiologists who work for the public health agencies were honest and looked at the data.
Now I know better. They fire you and silence you. And sometimes, they’ll even press criminal charges too like they did with New Zealand data whistleblower Barry Young.
It’s simple: if you oppose the narrative, you lose your job. Watch this interview I did with former Hawaii public health epidemiologist/virologist Jennifer Smith or check out her book on Amazon Pandemic in Paradise.
And did you know that in Hawaii, their vaccine tracking system was completely out of service for 5 years and they didn’t let anyone know? And that even today, there are loads of paper documents that still haven’t been input into computers? This is another reason they hide the data from the public: so it isn’t apparent that they don’t have the data needed to make any of the public assurances that they made.


Next steps for me
Write this up for scientific literature.
Publish on a preprint server
Submit to high impact journal
When it gets rejected by all the top journals, submit to an honest journal
Next steps for Congress
Order the FDA and CDC take the mRNA vaccines off the market or to immediately show cause as to why that should not be done.
Request that the FDA and CDC apologize to the American public for approving vaccines that killed around 1M Americans.
Create a joint resolution asking President Biden to immediately replace the heads of the CDC and FDA with qualified individuals who publicly called out the COVID vaccines as being unsafe prior to 2024.
Drop the liability protection for all vaccine manufacturers now, not just the COVID vaccines. Doctors are taught in medical school vaccines are the safest of all medical interventions. It’s time to walk the talk. So why do they need liability protection when other drugs do not? Liability protection is simply an unlimited license to kill. I just don’t get it. It makes no sense.
Stop all government censorship related to medical matters.
Compensate the vaccine injured/dead.
Investigate the Maddie de Garay case.. Why was she never called? Why was the paper never retracted? What caused Maddie’s injuries if it wasn’t related to the vaccine.
Instruct the FDA and CDC to appoint new outside committee members chosen exclusively from those people who spoke out against the COVID vaccines, lockdowns, mandates, mandates and masking.
Require data transparency: the states should supply the info to the CDC who should then make the data publicly available.
Next steps for health authorities
Ask the drug companies to explain how this data shows their vaccines are safe and effective. If they cannot do that, revoke approval.
Update your websites to convey the truth. For example, the HHS website is very misleading by saying the vaccines are “safe and effective.” Simply add the word “NOT” in front of safe, effective. It’s an easy change.

Publish your record level data just like the Czech Republic did and publicly urge other health agencies to do the same.
Urge lawmakers to drop laws requiring vaccination to attend school. After all, if the medical community was so wrong on this one, their previous recommendations now need to be re-examined. In the meantime, we need to put a moratorium on mandates.
Apologize profusely to the public for giving advice that has injured and killed so many people. Blame the CDC and FDA.
Call out the state licensing boards and medical boards for their attacks on doctors who were speaking out to save lives.

How you can make a difference is easy. DO NOT re-elect President Biden.
President Biden pushed these dangerous vaccines on Americans.
He even tried to mandate that people be injected with them.
He ordered the military to require COVID vaccination.
He is responsible for the deaths and serious injuries of millions of Americans who trusted him. Countless children died, families were left with one or no parents, formerly healthy people are now so seriously injured they cannot work, and the list goes on and on.
Not only that, he supported the censoring of people who were trying to tell people the truth.
Look how CNN is distorting the truth and trying to make Trump look bad
My article shows, without a doubt, the medical community and regulators all pushed these deadly vaccines on an unsuspecting public.
And look how CNN is trying to convince you that President Trump doesn’t know what he’s talking about when Trump questions the safety of vaccines.

CNN is telling you that Trump is wrong and the vaccines have been proven “safe and effective through rigorous scientific study.”
Are you kidding me??
And then they say vaccines conclusively do not cause autism. Another big fat lie. There are no debates on this issue because nobody who believes this will consent to debate the experts who disagree. If vaccines don’t cause autism, then why was CDC scientist William Thompson ORDERED by his CDC bosses to DESTROY all documents that proved that it did? How can pediatrician Doug Hulstedt have 44 kids turn autistic within 1 week AFTER their vaccine appointment, yet none turn autistic in the week prior their vaccine appointment. NOBODY CAN EXPLAIN THAT. It’s in the medical records that nobody wants to look at!
Look at this article published today from Aaron Siri about the Moderna clinical trial data that is NOW FINALLY COMING TO THE SURFACE! It says, “The latest batches of Moderna COVID-19 vaccine clinical trial documents continue to show that participants had a significant number of medical emergencies—including death, heart surgery, cancer, and miscarriage—in the days and months following vaccination. These crucial documents are reluctantly being produced by FDA at an average rate of 180,000 pages per month, after the attorneys who represent ICAN won a lawsuit in May 2023.”
It had to take a lawsuit to force public disclosure of documents showing the FDA looked the other way at all the adverse events that showed up in the clinical trials in 2020.
Please consider supporting my work to expose the truth
If you like my work and want to say “thanks” for the 1,500 Substack articles exposing the corruption over the past 3 years, please consider subscribing for just $5/mo or $50/year. I’d appreciate it as it enables me to afford to focus full time on creating articles like this one that expose the truth and help save lives. Thanks!!
Summary
For the first time in world history, we have gold-standard government data that was made public that allows us to compare the safety of the different COVID vaccine brands.
Today, the truth is in plain sight for anyone with an open mind to see the truth, download the data, replicate the analysis, and realize they were fooled.
The source data can’t be attacked. The method cannot be attacked. The data analysis has been independently replicated. The interpretation is brain dead simple. There are no viable alternative explanations other than the vaccines were unequally deadly.
It simply doesn’t get any better than this data.
More importantly, it shows that the medical community is inept when it comes to safety monitoring of vaccines. The regulators had the data but kept it hidden from public view and never looked at it. The medical community never asked to see the data.
With this data release, the cat is now out of the bag.
The fact that they have not been able to find a safety signal this large in over 3.5 years is inexcusable. They need to take a hard look at how they failed. In the meantime, they should immediately call for a halt to the mRNA COVID vaccines worldwide, a moratorium of all vaccine mandates for other vaccine types (such as mandating kids get vaccinated to attend school), the end of liability protection for vaccine manufacturers, full data transparency for all vaccines that are approved in the country, and demand compensation for those doctors who have been victimized by the medical boards and state medical licensing authorities for speaking the truth.
Honest political leaders should require that their public health departments immediately disclose their record level with the same level of detail as the Czech data. This does not require new legislation. Disclosing this data would immediately reveal the truth and save countless lives. We cannot do this through FOIA requests because public health agencies can use all kinds of legal loopholes to deny the requests.
Sadly, most of these leaders are more interested in protecting their reputation than in saving lives of the people they serve.
Thank you to US Senator Ron Johnson, former UK MP Andrew Bridgen, Dr. Peter McCullough, Dr. Robert Malone, Dr. Paul Marik, Dr. Pierre Kory, Dr. Bret Weinstein, Dr. Chris Martenson, Del Bigtree, Aaron Siri, Dr. Jessica Rose, Dr. Joe Ladapo, Russell Brand, Tucker Carlson, Joe Rogan, Naomi Wolf, Dr. George Fareed, Dr. Brian Tyson, Dr. Meryl Nass, and so many others for having the courage to speak the truth and oppose the false government narratives.
This data is a powerful new tool that should convince anyone with an open mind and scientific background that they have been misled by the authorities and that millions of people have paid the price with their health or their lives.
“I don’t know of a single person who has stated the vaccines are unsafe who has switched to the other side. Can you name one?” — Similarly, I suppose you might just as easily have written “I don’t know of a single person who has declined getting jabbed who has regretted doing so.”
I’m so grateful for your fact-based work, authenticity and dedication. So many people have been fooled, injured, and so many have died tragically—while the companies rake in billions for their dangerous products. Every person suffering or dead as a result of these products matters. Their circle of pain, suffering and death is vast. Where is the tipping point to stop this heinous cruelty towards humans?